The tide
has turned on chronic pain management.
Anyone who follows the media in any capacity will have seen this shift
particularly in regards to opioid medication with regular mentions of
addiction, and the harm it can do. What
generally is getting left behind in this discussion is patients with chronic
pain and the harm untreated pain can also do.
The very few appointments I’ve had with Pain Consultants in the last few years have also had a tone change. It’s gone from a dismissive ‘there’s nothing we can do for you so you need to live with it and manage the pain as best you can with the medications you are on’, to a very similar one that includes a long lecture about the need to reduce the medications I’m on. Ah, because of the side effects? No, that’s not the reason. Because I’m abusing them? Not at all – I’ve taken the same medication at the same dose as prescribed for many years.
No
alternative is offered. I’m not told about any of the latest research or
studies on pain reduction. I’m simply
told it would be best if I reduced my pain relief. I then counter with a
question about quality of life – how am I meant to function with an incredibly
painful condition with no pain relief? It’s a question that never gets
answered.
I have been
under the same Pain Clinic since I developed chronic pain at age 15 and I’m now
in my 30s. So I have now been in
constant, crippling pain for over half my life – and in that time nothing has
changed. There have been no new treatments offered after exhausting the very
little allowed Physiotherapy and Hydrotherapy on offer. I personally spent many years and a lot of
money trying every therapy I could find – from exercise-based to stretching,
sticking needles in me, to weird off-beat ones, ones that target the mind and
many in-between. The NHS, however, has
offered the same few inadequate options.
While I’m
sure research and studies go on in the field of pain – I don’t keep up with
them at all. This may seem strange to
those without pain – but it would simply be a heartbreaking way to spend my
time. Even if there is a miraculous breakthrough, having that get through all
the trials, work for all patients with pain, be funded and offered by somewhere
I can access are all huge steps to climb.
The
judgement always feels like it’s on the patients to be doing something
differently. Self-management. How I’ve come to loathe that term. If cards were dealt to chronic pain patients
– self-management should just be one in their hand, along with Specialist
Consultant, Psychological Support, Care Needs, Equipment, Treatment Options,
Medication and I’m sure you can think of many others. What it feels like
instead is the NHS has either run out of cards to give or have taken the rest
away, so the patient gets left with one single option of self-management and
are told to like it, or lump it.
I’ve had
many of those other cards ripped away from me, but I’m still clinging on to my
medication card. I feel judged for doing so and more importantly, I feel
scared. Every time a new report comes out about opioid medication and addiction,
I wonder what the impact will be on chronic pain sufferers. Of course addiction
happens, and I’m not suggesting it’s an issue that should be ignored – but
instead it’s those of us with incurable painful conditions simply being left
out of the equation instead.
There are
such amazing advances taking place in medicine, but the knowledge we have of
both pain and pain relief still feel so basic.
How much money and research actually takes place in creating non-harmful
painkillers?
The UK
should not follow the same approach as the US that has villainised chronic pain
patients. It seems many Pain Clinics in the US now have a blanket ban on
prescribing pain relief, and will not take patients that have existing
prescriptions. For the very few that do allow medications, they will often make
patients sign a contract with them that has numerous restrictions such as
spot-check urine tests and the fact the patient is simply not allowed to take
anything other than their prescription. While it may seem reasonable on the
surface – this can include patients having to refuse pain relief after
accidents, operations or similar. People
with complex conditions can metabolise medications differently, and I’ve seen
cases where people who took what was prescribed having their prescription
revoked because their urine test either showed not enough or too much in their
system even though they were taking what they were supposed to. Other patients have had to stop taking
cannabis or CBD oils used legally that they found helpful because their contract
had a blanket ban on them.
Not only do
patients find the contracts stressful and coercive (i.e. they have to sign them
to receive any pain relief) a 2010 review also found that evidence was weak
that these contracts actually reduced misuse of medications.
I
personally believe it should be basic care to receive adequate pain relief, and when it’s treated this way the
relationship between patient and doctor simply becomes both negative and
fearful. An article in the British Medical Journal states, “One systematic
review suggested that addiction occurs in 8%–12% of individuals taking prescription
opioids, but most data in the review derive from the USA and we have no
definitive figures for European populations.” So not only are a lot of fears of
addiction coming from data in the US where the addiction rates are simply
higher, then even taking the figure from the US of 12% it still means a huge
majority are taking the medication correctly and as prescribed.
Generally
both chronic pain and Pain Clinics in the UK are an underfunded and
underresourced area. Just taking my local hospital alone five years ago the
clinic had eight full-time consultants, two pain nurses, a pain psychologist
and numerous support groups and pain management groups that were run
weekly. From that list, all that remains
is one part-time consultant. The rest have
simply vanished. Yet rates of chronic
pain patients and their needs have not gone away.
If the NHS wish
to reduce the use of painkillers they need to offer well-funded Pain Clinics
that can offer an array of services and alternatives in return. They can’t
remove both the clinics and pain relief and expect patients to just ‘get on
with it’. The result will simply cause
far more of a burden on other medical and care services as patients deteriorate,
and there will almost definitely be a massive increase in chronic pain related
suicides.
Yesterday I went to London to see Dr Hakim, one of the top specialists in Britain for Ehlers-Danlos Syndrome.
I was nervous when I got there – I always am before I see a consultant, due to many, many bad experiences. However he immediately put me at ease, and was a nice, approachable person.
I’d made a list of problems I wanted to talk about, and he made a note of them and went through each in turn giving me ideas and suggestions of particular treatments or medications I could try.
He said in terms of exercise I was doing everything right, and everything I could. This meant a lot, as I’ve had medical professionals be so judgmental with no understanding of how hard it is to do the ‘little’ I do without putting myself in bed for weeks. I told him what one Pain Consultant had said – that I should be exercising six times a day. He said it was such an easy thing to say, and proved how little he knows.
We spoke about my Physiotherapist Leon Stephens at Sudbury Physiotherapy Centre who specialises in Hypermobility, and has been great, and Dr Hakim knew of him, which was good.
At some point this year I need to renew my Employment and Support Allowance, and in the next couple of years my indefinite Disability Living Allowance award will be changed over to the replacement – Personal Independence Payment (PIP). I’m terrified about both of these, as are most disabled people in the country who currently rely on them – or may need them in the future – to survive. I never know how people may react to something like that, due all the ‘scroungers’ rhetoric in the media, that has been picked up by so many.
Since I received my diagnosis letter in 2011 – I haven’t had a decent letter from a consultant that I could use as medical evidence. I’ve seen lots of consultants, but letters are generally of the “Treatment x didn’t work, been discharged” variety which won’t help much in terms of summarising where I’m currently at on the whole. I feared the lack of letters may go against me, as the Department of Work and Pensions will argue I can’t be that bad if I don’t see a consultant regularly.
Dr Hakim was very understanding of this, and we spoke at length about the PIP changeover, and he knew how hard it was on his patients. He said it’s obvious the reason I don’t have new evidence is because I’m doing the best I can at home to manage, but he would write an updated version for me to keep on file for when I need this.
This will take a huge worry away from me, so I’m thrilled.
He recommended that I take a multivitamin daily – he mentioned the Well Woman one, to make sure I’m topping up on anything that could be contributing to my levels of fatigue. He’s also going to ask my GP to check every blood test has been done, including the T3 Thyroid test that the NHS often miss out. He also suggested getting some Melatonin from the US, as well as suggesting some other sleep and pain medications I have yet to try that he’s going to suggest to my GP to look into (I can’t remember the name of them currently!) He also recommended some consultations in other fields that I could see if I continue to get nowhere locally.
He also suggested that anyone with POTs or autonomic dysfunction (including sleep problems) to drink an Isotonic drink called Nuun. He explained that they tell people like us to keep hydrated, so we drink water – but it actually make things worse as it dilutes the salt in our blood, so our kidneys then filter it and we pass it out with urine leaving things actually worse. (Or something like that!)
So he suggested drinking a salt isotonic drink which means that we are really hydrated, as drinking liquid with a similar salt content as our blood means it will do its job, rather than being filtered and disposed of straight away. Most of the similar products on the market i.e. sports drinks, Lucozade, etc are full of crap and sugar, so he suggests Nuun as it doesn’t add much else, just some flavouring. He suggested at a minimum to drink one before bed, and one as soon as you wake up, and this should stabilise some of those issues.
They are pretty expensive, but we only need half a tablet at a time, as the whole tablets are designed for athletes.
We also spoke about Prolotherapy, which is a new therapy I’m hearing a lot about recently, mostly from Americans, and I was interested in his thoughts. He said there was no evidence for it, and some of his patients had been made worse by it.
I found Dr Hakim very understanding, kind and obviously knowledgeable. All in all it was a great appointment – and when his letter arrives I will add anything helpful I’ve forgotten!
Professor Grahame retired from NHS patients some time ago, and is no longer taking on new private patients. I believe he may still have a private clinic for under 16s, but Dr Hakim is a perfect alternative.
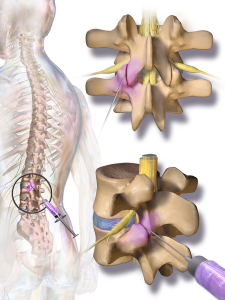
I have pain all over the place, but ranking at the top of the list is my lower back. I’d previously had facet joint injections in my neck and shoulders some years ago, but they didn’t help. However, it was before I’d had an MRI (as it took around 8 years of arguing to get one) and so the consultant was ‘guessing’ at what the issues were. Later on the MRI did clearly show an area in my lower back that had degenerative lumbar disease in the facet joints, arthritis, and others issues. It made a much better target for injections than anywhere else, so I thought it was worth a try.
It took another few years of me arguing for them (nothing ever just seems to just happen on the NHS!) After getting nowhere locally, my Ehlers-Danlos specialist at the Royal National Orthopaedic Hospital at Stanmore sent me to see her Pain Management college, who gave me the go-ahead for bilateral lumbar facet joints at L4/L5 and L5/S1 (so four in total).
A few days passed after being told I could have them and suddenly I thought – what the hell am I doing fighting to have needles put into my spine?! I was sedated during my previous injections, but I did have some memories of the procedure. I remember my consciousness kind of returning and thinking ‘please stop now.’ I was later told the sedation didn’t actually knock you out, but simply wiped your memory – and that you would be aware of what was happening as they did it. This memory built up in my mind until I was convinced I’d be strapped down with horrible painful injections into the middle of my spine, then I’d just forget afterwards so I didn’t realise how awful it would be. So I was about 500 times more nervous for these injections than previously.
The whole topic became a ‘do not discuss’ subject. As soon as I thought about it I went into a state of panic, so there was no research done as I normally would, and I didn’t even allow my mum (who accompanied me) to talk about our arrangements of getting there until the day before. I just wanted to block it totally from my mind.
We travelled to Stanmore the day before for two reasons. The first that I can’t make the journey there and back in one day, and the second was that my admission time was 7am. Ugh!
Although I wasn’t having general anaesthetic, I was told not eat after midnight, and no drinking after 6am. It was the latter I’d struggle with as I’m constantly thirsty.
I arrived at the hospital a couple of minutes before 7am and had a choice of parking for the first time ever! When we reached admissions there were a few people waiting outside, but when the queue got the doorway I realised the room was packed with both people queuing, and waiting in the chairs. It wasn’t the easiest getting my wheelchair in and out with no room for manoeuvring. There was only one member of staff dealing with everyone. The older lady in front of me didn’t speak any English, and was soon joined by an interpreter. The staff member made a phone call and I heard him say, “Are the wards still closed, there are a lot of patients here?” He then informed the interpreter they had a bit of a wait ahead. I was next, and was told the same thing.
I was a little cross, only because getting somewhere for 7am isn’t very easy for me and more importantly 7am = grumpiness! I did later found out the wards were opening for the first time after being closed for two weeks over Christmas – so I assume the delay isn’t normal.
I reached the ward and was met with a number of friendly nurses and health care assistants who welcomed me, and showed me my bed. The lady with the interpreter was in the bed opposite me. A nurse admitted me with a huge pile of paperwork, most of which seemed irrelevant in my case! I was asked a couple of times if I had any allergies. She then took swabs for MRSA and then took my blood pressure (which I hate, as it’s very painful. The muscles in my upper arm are very tight and particularly sensitive). I was told I was third in the queue – and the doctor would be seeing me beforehand.
A couple of other patients got in the bed and went to sleep, which seemed like a good idea – and would also make the time pass. However every time I was about to drift off I was woken by someone. The first to measure me for pressure stockings, then again to tell me I didn’t need them. Then a doctor who was working with my consultant arrived to explain the procedure. I was glad it was her and not my consultant as she was much warmer than my consultant is, which helped. She spent a lot of time explaining how much time they took to sterilise everything to reduce any chance of infection. I wanted to rudely interrupt and say that at that point, I didn’t care – I just wanted her to promise she’d knock me out! She then went through the possible risks – infection, numbness in the legs, pain flaring up afterwards and in a very tiny amount of cases nerve damage. She asked if I had any allergies.
Finally I could ask the one thing I wanted to know.
“You will be sedating me, right?”
“Did you ask for it before?”
“Yes,” I emphasised.
“Then we will.”
“Will I know what’s happening?”
“Well, some people do sleep.”
“Please make that happen with me. Please.”
Then the pharmacist came to take note of my list of medications, and asked whether I had any allergies, then a number of nurses came to tell me, “It won’t be much longer.” Then that they were on their way for me, only to still be there sometime later!
Eventually the porters did arrive and wheeled me into theatre. A nurse went through the final questions – checking I knew what procedure I was having, if I’d had any before, if I had any allergies and if it was definitely my signature on the consent form. The nice doctor then fitted the cannula into my hand, before I lay down front-first on the table. They put an oxygen mask on me, a clip onto my finger to measure oxygen (I’m sure that has a proper name) then to my annoyance – a blood pressure cuff which I was told would be taking my blood pressure every few minutes. It took it twice, before I told the nurse how painful it was. “No problem,” she told me cheerfully, and moved it onto my leg instead which was much better. She then began chatting to me about my hobbies and jewellery making, before my consultant began putting the sanitising fluids on my back. The nice doctor then began to input two injections of sedation into the cannula. I closed my eyes – trying to relax. She then asked if I could still hear her, and I said yes. She thought I’d gone to sleep, and I said I hadn’t felt any sedation yet. She said she’d keep going, and added two more tubes.
The next thing I remember is feeling a bit of pain in my back, and a nurse telling me it was all over. I definitely hadn’t been aware of it. I was taken into recovery for awhile, still very sleepy and groggy. A nurse chatted to me for awhile, and I remember telling her to say thank you to the nurses, as they’d calmed me down a lot beforehand. She promised she would. She then asked if I knew which ward I’d been in.
“It began with J…” I answered.
“Jackson Burrows is the only ward beginning with J.”
“No, it wasn’t that. Was it Diane something?”
“I guess now wasn’t the best time to test your memory?” she laughed. She then came back and said that unfortunately they’d moved me to Margaret Harte Ward. I began to worry if anyone had told my mum as I knew she was planning on getting a cup of tea while I was in the theatre (as she’d very kindly not eaten/drunk anything in front of me while I couldn’t).
As the porters wheeled me out of recovery, the nurse suddenly called for them to stop. She dug through a cupboard, and pulled out another blanket to put around me. “Sorry,” she said to the porters. “I just didn’t want her to get cold on the way back.”
When we got back to the ward I spotted my mum very quickly and realised it was the ward I’d been in all along! The nurse handed over to the ward nurse, and said that my blood pressure had risen quite a bit during the procedure, so they needed to keep an eye on it. Argh, more blood pressure checks!
I was left to sleep for a bit as I slowly came round. A nurse then came round to do the blood pressure test. I admit I groaned, and said the test was hurting quite a bit, then of course after gritting my teeth the machine malfunctioned. Just one more time, I was told. Luckily it was back to normal, and as she took the cuff off she realised lots of red marks had come up all the way round (which are still there today!). She gave me an apologetic pat. I asked if she could take my cannula out as it was pulling quite a bit. She took a look and said it was quite red, and that someone would do it before I left. (Well, one would hope so!)
I was told to stay until lunch time, and then I would be discharged. The nice nurse who admitted me then walked past and so I asked her about the cannula, and she said no problem and took it out. She also checked my ‘wounds’ (just slightly larger than needle marks) and said she was happy with how they looked.
Still waiting opposite me was the older lady with the interpreter. I heard a nurse say to her that her operation wasn’t going to be until mid-afternoon – yet she’d been admitted at 7am! It seemed mean to make her wait so long, and I assume the NHS had paid extra for the interpreter when they could had admitted her at the 11am or 2pm admission times. I noticed the little old lady chatted non-stop to her interpreter, which made me smile as I could just imagine in the 7+ hours the interpreter sat with her she got to hear her entire life story.
I left at 1:40pm, slept all the way home, slept all afternoon and very unusually for me – all night!
So all in all – it wasn’t nearly as bad as I dreaded. The staff – particularly the nurses, were lovely. There were lots of touches of kindness, like the nurse in the theatre distracting me from my nerves, the recovery nurse chatting to me as I came round and making sure I was warm, and the staff back on the ward who took care of me and offered me toast and regular drinks when I came round. They all made it a much easier experience. Also – the NHS really, really want to know if you have any allergies.
I’m in a lot of pain now which feels different to my usual pain. I was warned I may flare up, particularly where the needle touches the bone – so I’ve no idea if it worked yet. I think I need to wait for all of that to calm down over the next couple of days before I can tell if it helped.
I don’t tend to cry. I mean – give me a sad film, or book and I’m sobbing like nobody’s business. But in pain, randomly when it’s all just got too much? Not that often. (Although let’s take my last year of work out of the equation, because dear god I was a mess.)
But I have cried in my last three appointments, and all three times it was around the same topics. Frustration at the “system” and exercise.
The last few months have been tough for me. My condition seems to have gone into haywire, insomnia has struck big time, my pain levels are pretty damn ridonkulous and I’ve been pretty much stuck in the house. It’s always tough when you have a flare up, because of the fear this is your new reality. This is the next downward slide, on a slide that’s been pretty slippery for the last eleven years. At the same time there has to be hope. Sometimes I pin it on myself – I’m going to try this supplement, and do these new stretches eight times a day until every muscle in my body is strengthened and then…
And then I’m doing the most basic of basic stretches, and put my joint out, and I’m lying on the floor with half my body shaking in spasm, trying not to throw up and thinking if I can just make it back to the sofa and not move for five days, it will be okay.
So then I pin that hope on others. That I’m going to go to the physio and they’ll give me as much Hydrotherapy as I need, and then I’ll see the pain consultant and they’ll read the research I’ve found around a specific new medication that looks really promising and will give it to me without a fight, and then…
And then I’m sitting with the physiotherapy who is giving me the lecture that they don’t have infinite resources, so I can have one more block of hydrotherapy next year, and then that’s it. I’ll have to find somewhere else to go, and I’m trying to explain there is nowhere else, nowhere accessible, nowhere affordable, and I’m crying because I just want them to say yes, no problem, for once.
And then I’m at the pain consultant – the one that’s meant to work with people with Ehlers-Danlos Syndrome a lot, except she’s getting the most basic elements of the condition wrong. She does read the research I push at her, and she turns and says – “Yes, we do this here.” There’s a pause, my heart races. “But not for people with your condition.” And then she’s lecturing me – you need to exercise, and push through the pain, it can’t be that bad. And I’m trying to tell her, explain that I’m not talking about aching muscles the next day after a session at the gym, but agonising and consuming pain, partial dislocations – bedbound for days, and I’m crying because she doesn’t get it.
And then I’m at the osteopath, and she has her elbow in my lumbar spine, and she says, “Have you considered exercise?” And I sigh internally, but politely try to explain the same old issues, that I do exercise – but it has to be extremely limited, and she’s pushing it and pushing it until the tears are there again and then she’s backpedalling, and sorry.
It’s so frustrating, I hate crying – and on their own are such minor things. It’s the build up of it all, the feeling they’re just not listening.
But I need to wipe my tears, because it gets me nowhere, and push on with what I can. I’ll get there.
If you ask a doctor how to care for a chronic condition, or read their guidelines, or even go in hospital for a month on an intensive-pain management course (just to be specific) the themes running through them all, their little buzzword, is self-care.
I was reading the papers that have been created in the wake of the imminent closure of the PCTs by the doctors commissioning consortia whose priorities for the future are self-care, with aims to give patients the confidence to manage their conditions themselves.
To be fair, this may help with some conditions where perhaps a specific therapy or medication keeps symptoms at bay, but it gets a little more complicated when it comes to complex conditions where pain and fatigue are two pervading symptoms, amongst many others, because there is no single treatment. There isn’t even ten treatments they can say hand on heart would help everyone with chronic pain.
To be frank, it infuriates me to hear phrases such as ‘take control of your own treatment’ or ‘You have the power in your hands’ etc, etc, blah, blah, blah.
What they don’t tell you is that you have to. Self-care, that is. Because it will make up 99.9% of your overall treatment plan. Oh, it may be occasionally the NHS will think of something – physiotherapy injections, uhh… more physiotherapy, that is if you kick up enough fuss. Otherwise, it’s DIY all the way.
At the age of 15 I visited a Rheumatologist. He said I’d ‘grow out of it’. In the following years I was sent a couple of times for Physiotherapy, but it didn’t make the slightest bit of difference. The NHS then gave up, and in desperation I saw chiropractors, osteopaths, acupuncturists and electro-acupuncturists. I tried the many sheets of exercises and stretches, swimming and pilates and a GP referral to the gym (that I paid for) which put me in bed for two weeks. I then started the ‘alternative’ stuff like the Alexander Technique to improve posture, the Bowen Technique which seemed weird and pointless. I saw Kinesiologists and had relaxation sessions. The only tiny bit of relief came from the many thousands of massage treatments I once again paid for.
I’ve researched madly, kept up to date with papers on pain, studies on medication, and constantly visit the doctor with a new research paper in hand.
I even diagnosed myself – after years of consultants shrugging their shoulders at me, I kept searching and searching until I finally realised what was wrong with me, and then fought to see consultants in London who finally knew what they were talking about.
I now can only exist and function from a mixture of massage and adjustments, which takes the edge off – maybe 5-10% at best. But it’s an important percentage.
In the ten years I’ve been madly trying anything and everything, the NHS gave me one set of facet joint injections in 2008. Some muscle injections in 2011. And six sessions of Hydrotherapy – but I had to fight for them all.
The thing I find infuriating is that no one tells you exactly what IS available. I had severe back problems for ten years before someone said to me there was a spine clinic in my town for people with long-term back issues. Do you really have to hit the ten year mark before they go crap, that is long term for a twenty-four year old?
When you get a diagnosis no one gives you a handbook and says here is what the Pain Clinic offer (if they deem you lucky enough to offer you anything at all) or let you know you can see Osteopaths and Chiropractors on the NHS. Or any other of the treatments they may have available. You have to wait until you stumble upon it yourself.
All they do is hand out painkillers (again, if you are lucky) and tell you self-care is the way it should be.
Sometimes I want to say you know what? I’ve self-cared. NHS – it’s your goddamn turn. I’m just too tired.