The tide
has turned on chronic pain management.
Anyone who follows the media in any capacity will have seen this shift
particularly in regards to opioid medication with regular mentions of
addiction, and the harm it can do. What
generally is getting left behind in this discussion is patients with chronic
pain and the harm untreated pain can also do.
The very few appointments I’ve had with Pain Consultants in the last few years have also had a tone change. It’s gone from a dismissive ‘there’s nothing we can do for you so you need to live with it and manage the pain as best you can with the medications you are on’, to a very similar one that includes a long lecture about the need to reduce the medications I’m on. Ah, because of the side effects? No, that’s not the reason. Because I’m abusing them? Not at all – I’ve taken the same medication at the same dose as prescribed for many years.
No
alternative is offered. I’m not told about any of the latest research or
studies on pain reduction. I’m simply
told it would be best if I reduced my pain relief. I then counter with a
question about quality of life – how am I meant to function with an incredibly
painful condition with no pain relief? It’s a question that never gets
answered.
I have been
under the same Pain Clinic since I developed chronic pain at age 15 and I’m now
in my 30s. So I have now been in
constant, crippling pain for over half my life – and in that time nothing has
changed. There have been no new treatments offered after exhausting the very
little allowed Physiotherapy and Hydrotherapy on offer. I personally spent many years and a lot of
money trying every therapy I could find – from exercise-based to stretching,
sticking needles in me, to weird off-beat ones, ones that target the mind and
many in-between. The NHS, however, has
offered the same few inadequate options.
While I’m
sure research and studies go on in the field of pain – I don’t keep up with
them at all. This may seem strange to
those without pain – but it would simply be a heartbreaking way to spend my
time. Even if there is a miraculous breakthrough, having that get through all
the trials, work for all patients with pain, be funded and offered by somewhere
I can access are all huge steps to climb.
The
judgement always feels like it’s on the patients to be doing something
differently. Self-management. How I’ve come to loathe that term. If cards were dealt to chronic pain patients
– self-management should just be one in their hand, along with Specialist
Consultant, Psychological Support, Care Needs, Equipment, Treatment Options,
Medication and I’m sure you can think of many others. What it feels like
instead is the NHS has either run out of cards to give or have taken the rest
away, so the patient gets left with one single option of self-management and
are told to like it, or lump it.
I’ve had
many of those other cards ripped away from me, but I’m still clinging on to my
medication card. I feel judged for doing so and more importantly, I feel
scared. Every time a new report comes out about opioid medication and addiction,
I wonder what the impact will be on chronic pain sufferers. Of course addiction
happens, and I’m not suggesting it’s an issue that should be ignored – but
instead it’s those of us with incurable painful conditions simply being left
out of the equation instead.
There are
such amazing advances taking place in medicine, but the knowledge we have of
both pain and pain relief still feel so basic.
How much money and research actually takes place in creating non-harmful
painkillers?
The UK
should not follow the same approach as the US that has villainised chronic pain
patients. It seems many Pain Clinics in the US now have a blanket ban on
prescribing pain relief, and will not take patients that have existing
prescriptions. For the very few that do allow medications, they will often make
patients sign a contract with them that has numerous restrictions such as
spot-check urine tests and the fact the patient is simply not allowed to take
anything other than their prescription. While it may seem reasonable on the
surface – this can include patients having to refuse pain relief after
accidents, operations or similar. People
with complex conditions can metabolise medications differently, and I’ve seen
cases where people who took what was prescribed having their prescription
revoked because their urine test either showed not enough or too much in their
system even though they were taking what they were supposed to. Other patients have had to stop taking
cannabis or CBD oils used legally that they found helpful because their contract
had a blanket ban on them.
Not only do
patients find the contracts stressful and coercive (i.e. they have to sign them
to receive any pain relief) a 2010 review also found that evidence was weak
that these contracts actually reduced misuse of medications.
I
personally believe it should be basic care to receive adequate pain relief, and when it’s treated this way the
relationship between patient and doctor simply becomes both negative and
fearful. An article in the British Medical Journal states, “One systematic
review suggested that addiction occurs in 8%–12% of individuals taking prescription
opioids, but most data in the review derive from the USA and we have no
definitive figures for European populations.” So not only are a lot of fears of
addiction coming from data in the US where the addiction rates are simply
higher, then even taking the figure from the US of 12% it still means a huge
majority are taking the medication correctly and as prescribed.
Generally
both chronic pain and Pain Clinics in the UK are an underfunded and
underresourced area. Just taking my local hospital alone five years ago the
clinic had eight full-time consultants, two pain nurses, a pain psychologist
and numerous support groups and pain management groups that were run
weekly. From that list, all that remains
is one part-time consultant. The rest have
simply vanished. Yet rates of chronic
pain patients and their needs have not gone away.
If the NHS wish
to reduce the use of painkillers they need to offer well-funded Pain Clinics
that can offer an array of services and alternatives in return. They can’t
remove both the clinics and pain relief and expect patients to just ‘get on
with it’. The result will simply cause
far more of a burden on other medical and care services as patients deteriorate,
and there will almost definitely be a massive increase in chronic pain related
suicides.
First of all sincere apologies for the lack of updates lately. It’s been such a busy time, that writing has fallen by the way-side a little.
I just thought I’d give you a small update about what I’ve been up to lately.
I recently wrote about the process of obtaining a Personal Budget to employ a Personal Assistant. I’ve had that in place a couple of months now, and it’s been brilliant. She’s been able to help with a range of things, from the obvious helping with care, but also driving me to appointments, getting my wheelchair out, cooking, sorting out areas I haven’t been well enough to do in my home, etc. It’s taken quite a bit of stress out of my life and I’d recommend it to anyone.
Medically I’m still very much in no-man’s land. The Pain Clinic have declared me incurable and untreatable, and discharged me. Apparently they only help people who will get better, they’re not interested in actually managing pain. My specialist consultants also are no longer able to keep me on their books due to over-subscription, so I’m consultant-less. It’s quite a scary place to be.
My GP has been trying to help with this situation, and wrote to a local Rheumatologist who lists himself as a connective tissue specialist on the hospital website. He rejected my referral, and wrote back saying, “I have no interest in managing Ehlers-Danlos Syndrome.” Although he did refer me to a Hypermobility Specialist Physiotherapist instead. Silly, silly me actually got my hopes up and thought she might be interested in working with me to move forward. Instead without any examination she declared there was nothing she could do, so I’d have my final batch of Hydrotherapy and that would be it. She then spent the rest of the session basically telling me I should be perfectly okay in the mornings, as other people with the condition manage. I tried to explain I have severe insomnia and sleep issues, and am a total mess in the mornings, but she wasn’t interested.
I then finished my final block of Hydrotherapy, which I really enjoyed. I do find the warmth means I can do much more than out of water. I would love this on a rolling-basis, and will keep trying to pester the hospital to make this happen.
I’ve also just had a sleep study done, but I’m waiting for the results. It was a machine I had to take home, that strapped to my stomach and chest, a tube went up the nose (nice!), a mask for your mouth and finally a clip for your finger. They have to rule out Sleep Apnoea before they’ll send you to a sleep consultant, but I am a little worried they’ll tell me it’s not Sleep Apnoea, and then not let me see anyone at all. Hopefully I’ll get the results soon, and this long-term issue is explored.
I have been lucky enough to find a private physiotherapist, however, that has an interest in Ehlers-Danlos Syndrome – and he genuinely does. It’s a lot of money, but the only treatment I’m now getting. He hasn’t promised he will be able to help me, but he’s going to try. If I can even maintain what little mobility I have, that would be a start. I’m diligently doing all the exercises he’s giving me (not a hurriedly printed out sheet, but thoughtfully targeting specific issues) and he’s easy to contact if things go wrong to provide advice, and alternative exercises. He really seems to know his stuff, so that’s been great.
I also recently took part in a study on Ehlers-Danlos Syndrome that’s all about what triggers the condition in the first place (obviously it’s genetic, but there is often an occurrence in your life that makes it much worse, often puberty, having children, an accident or something else. Others just have it severely from birth, so it’s exploring all of that.) The research also looks at flare-ups and the triggers.
The research sounds really interesting, and when it’s published it will obviously go into medical journals, but particularly GP and physiotherapist journals, to catch front-line staff.
One thing I truly believe is that the fight for decent rates of diagnosis lays almost entirely with GPs and Physiotherapists. They’re the ones that have to see signs, and see past one problem joint, or a history of chronic pain without a solid diagnosis and make a referral to a specialist. Once they have that awareness, only then can diagnosis rates climb.
I’m also preparing for Christmas, and this year have decided to have my first ever real Christmas Tree! I’ve also been making festive bunting with the help from my Personal Assistant, and it’s the first year in a really long time I’ve been genuinely excited for Christmas!
Please comment below to tell me your news, and whether you’re looking forward to Christmas or not?
My mum is currently having physiotherapy after an operation on her shoulder. She got chatting to her physiotherapist, and my condition came up – Ehlers-Danlos Syndrome. It turned out that the physiotherapist has a great interest in the condition, has a few patients with it, and leads the in-house training to the other physiotherapists. She invited me to come along to give a talk to them during that session.
So that’s how I ended up pretty much taking over the whole training session myself.
The idea originally was that the physiotherapist would cover the medical and exercise aspects, and I would cover the daily living aspects – but my notes grew longer and longer. This was my chance to help make things better for people with the condition, and there was so much to say!
When you speak to someone with EDS, or other complex chronic conditions you’ll often find that they have had a bad history with a physiotherapist at least once in their past, and sometimes repeatedly. (Here are just two posts talking about previous experiences here and here.) But sometimes it’s not their fault – we are well aware they have to see a lot of people in not a lot of time, and are generally encouraged to discharge as soon as possible. Many report being asked to pick one joint that is the worst, being handed a couple of exercise sheets and that being the extent of their treatment. Others, including myself, saw physiotherapists for years without them ever mentioning the hypermobility – that could have led me to that crucial diagnosis.
While I had a lot I want to say myself, I wanted to let other people with the condition have a say as well.
So I went on to a Facebook group that has over 5000 people with the condition on and asked them what they would like to say to physiotherapists if they could. From that, adding in information about our symptoms, our daily lives, the different types and so on, I built up a talk.
The way their training sessions work is that they have an hour built into the day, and all the physiotherapists who don’t have a patient at that time, come along. She expected around 4 to 5 to attend – but when I arrived I was faced with a very small office filled with around 10 physiotherapists. It wasn’t so long ago I would have immediately turned my chair around, found a toilet and locked myself in it until they all went away, but I’m very lucky that over the past few years I’ve been chairing a meeting group and have greatly gained confidence in public speaking – to a certain extent, I’m not saying I’d be happy to give a speech to a large amount of people, let’s not get silly here.
It also helped I was talking about something I was passionate about – the education of front-line medical professionals.
A few of the topics I spoke about included the difference between Ehlers-Danlos Syndrome, Hypermobility Syndrome and Benign Joint Hypermobility Syndrome. A general overview of how many medical professionals and consultants someone with EDS sees before they get a diagnosis, and the fact that it takes 30% of patients over 10 years to receive a diagnosis of EDS and over 20 years to 50% of patients. I also emphasised the fact that 95% of patients remain undiagnosed or misdiagnosed. I also spoke about which conditions are most commonly diagnosed instead of the correct or underlying cause of EDS, and also gave some tips in what not to do when treating or examining someone with the condition. I particularly emphasised that the condition is extremely variable – and that if we can’t come to a session or a few sessions it doesn’t mean we are uninterested, or lazy – just that it’s not what we are able to do at that moment. And it also depends on which areas of our body are a particular problem at the time, one week an exercise might be fine, but the next week dislocate a joint.
I emphasised to them that the way forward is for more frontline professionals to have an understanding of EDS – particularly GPs and physiotherapists who are often the ones patients see first.
No one expects everyone at those two groups to have full knowledge of the condition, when there are so many conditions out there – but it would be brilliant if when presented with a patient with long-term chronic pain, and hypermobility they referred them onto a specialist. Other things that would help patients is long term care, not just the six sessions that are offered on the NHS before being discharged, and the same thing with hydrotherapy, which should be an on-going treatment, particularly as it can be one of the only treatments that is effective for people with EDS.
They seemed interested, engaged with what I was saying, asked questions, and even asked advice on past cases and whether their care was appropriate (whilst maintaining confidentiality of course). One physiotherapist said that in general physiotherapists like regimented care, i.e. they can pick up a file for a patient that says they are currently doing six reps of exercise 1, and 10 of exercise 2, and so on. Any other physiotherapist could then pick up that folder and continue their care if needed. However when he had a previous patient with EDS he found that it was completely impossible to treat him in this way. One week he could do a decent amount, but the next all he could do is lay on a table whilst the physio mobilised his joints for him. Other sessions he couldn’t even make it to the hospital at all. He said that he had to be really flexible with the patient – which emphasised what I was saying.
I also told them about my previous physiotherapy sessions, where I spent the first session explaining how I might not be able to make every session, I was having a lot of flare ups and spending a lot more time in bed unable to do anything and she seemed really understanding. And then it happened, I had to cancel a session and it turned into a few weeks as it was a really bad flare up, and I called to update her and they said just call back when you’re ready, which I did, only to find that she had discharged me.
I was too exhausted to go back to the beginning, so just went without.
Another physio suggested that on occasions like that it would be helpful for the physiotherapist to visit me at home, but of course I’ve never been offered anything like that. Also when talking about ongoing hydrotherapy, which I have been told previously is impossible due to the waiting list – they informed me they do have a few rolling programmes, including one for paediatrics with hypermobility, and another for people with Rheumatoid Arthritis – so it is possible. I’ve now got the name of the manager, and I’m going to contact her and explain how important it is for this to be put into place – particularly when a lot of us are being told that the ‘land based programmes’, as they call them, are inappropriate for us.
Hydrotherapy, for a lot of people with EDS is very good because the water supports the joints, so dislocations are less, the warmth helps with the spasming muscles and we generally find we can do a lot more in the water. Of course this doesn’t apply to everyone, particularly if they have bad POTs alongside, as the heat can cause havoc with feeling faint and dizzy.
In summary I really enjoyed giving this talk, and have been invited back in July.
Patients talking to medical professionals is the way forward t0 them gaining an understanding to the reality of life with a complex condition, without reading a little paragraph in a textbook.
So I commend the physiotherapist that setting this up, and I hope more will do so in the future.
Have you ever has an opportunity to talk to medical staff in this way? What would you have said?
I wanted to write about my experiences with acne and the route I took to try Isotretinoin/Accutane, as acne isn’t always something that gets talked about past your teenage years.
I was lucky enough to escape my teens with clear skin. Clearly karma said “screw that” and decided to smack me with it in my mid-twenties. I’m not entirely sure of the cause – but a consultant suggested it was likely due to the morphine messing with my hormones. This seemed very likely due to the placement of mine – the lower cheeks/chin, and the cyclical nature of them. Just as one lot were fading, the next lot would appear.
Acne can really hit your self-confidence. I was so embarrassed I found myself putting layer, after layer of foundation on to try and cover it – which just looked a mess. I tried lots of different foundations/concealers in my quest to tone down the redness, and for a long time wore Estee Lauder Double Wear – but found it slightly too dark for my skin tone. The best I’ve found is Bare Minerals, as you can easily add to areas that need coverage, while leaving the clear areas looking much better.
If you ask most acne sufferers what percentage of spots cover their face, they’ll often say 70-80%. But in most cases, even in pretty bad cases – it’s a far, far lower figure. The spots often group in specific locations, or have a number of bad spots that draw the attention and the rest of the skin tends to be clear, yet the spots are all the acne suffer focuses in on.
After trying various different off-the-shelf treatments, I went to my GP where I then tried every lotion and potion available on the NHS. You tend to begin with Isotrexin gel – which contains vitamin A and an antibiotic, and then go onto something like PanOxyl – in a wash or cream form, which contains benzoyl peroxide.
When these failed I tried asking other people with acne what worked for them. I first tried Living Nature, a range from New Zealand that contains manuka honey, which did nothing. I then spent a fortune on Dermalogica products – which at first perhaps cleared the latest batch slightly quicker than usual, but after awhile didn’t even do that.
Back at the GP she started me on various long-term antibiotics, each of which failed – including the ones that are used when it’s being particularly stubborn.
The problem with all the treatments is you have to try them for months, some of them aren’t deemed to be a failure until over six months have passed. Finally I’d exhausted every treatment a GP can offer – and met the policy of having acne for over two years that has caused scarring, which enabled me to be referred to a Dermatologist Consultant.
I knew there was only one option left – the medication now called Isotretinoin, but originally known as Accutane and then Roaccutane. I’d heard about it before – there had previously been some controversy about it possibly causing depression, and even suicide. I researched this beforehand, and decided the risk seemed minimal. The information I found suggested that people with long-term acne were generally more prone to depression, and it was highly unlikely it was linked to the medication.
However it seemed like my only option left, and said it particularly worked well for women with hormal-related acne, and with one course usually gets rid of it entirely forever. There’s a good overview of the medication here at Fashioninsta.
The consultant explained there were a few things I had to remember:
I would get dry skin
Not to get pregnant, as it would cause birth defects
Not to wax, as it would rip off the skin (nice!)
To wear sun lotion – as I would burn more easily. (I’m already a person that can burn while indoors!)
Not to drink alcohol.
He also said he had to warn me of other possible side effects of increased pain and depression, but they almost certainly wouldn’t happen.
I was then given two options – I could have a monthly pregnancy test, or I had to sign a waiver that agreed I would remain on birth control, and if I got pregnant it was my own stupid fault and I knew the risks. I did the latter.
I was also told that the medication could increase cholesterol, so I had to undergo a blood test that checked this along with my kidney function. Both were fine, so I was given the go ahead. My course is for four months – although I hope to speak about extending it, because I’ve heard that once the acne is cleared up, taking it one more month can help reduce the scarring. I don’t know if that’s true or not, though.
The first prescription was for a month, and then after that I have to return to the dermatology nurse every six weeks to check the side effects. I began taking three capsules (60mg) and the first month was fine – just a little bit of dry skin. After a month the dose was increased to 80mg, and the dry skin got quite a bit worse. It started on my lips, and then one day looked down and was surprised to find my arms had very suddenly turned scaly – like when it heals after a bad sun burn! I treated it with moisturiser, and my lips with Vaseline.
The symptoms got a lot worse when I hit the maximum dose of 100mg – a rash covered my arms, and then a few weeks later my legs. It’s red, and looks like tiny blisters. My arms and legs have become very sensitive, and now burns if I put moisturiser on. At one point it began to itch, so I put a antihistamine cream on. Big mistake – it felt like my skin had set itself on fire, but it sneakily took awhile for the feeling to start, so by then I’d coated both arms and legs. Whoops. The skin is also healing slower, there are red marks in places, and larger patches of dryness – particularly after I take my morphine patch off.
The rash on my arm after it had calmed down slightly
But pain also struck – very different to my usual every day chronic pain. This was an extreme stiff feeling in my joints, leaving me to shuffle along. The medication clearly dries out your skin, and it felt like it dried out my joints too! The pain was pretty awful for a couple of weeks, until I gave in and put the dose back down to 80mg. I haven’t gone up since then, and I hope 80mg is enough to do it. It may be people without pre-existing health issues/chronic pain may be fine on the 100mg dose. The pain lessened – although hasn’t gone, but the dry skin/rash, etc still remains. I also upgraded the vaseline to an intensive lip moisturiser – which is constantly reapplied.
I am now ten weeks into the treatment. I’ve heard the biggest changes happen from month three – four. At the moment my skin is looking better – I have two bad areas left, but the whole area has red non-raised spots still, so it doesn’t look clear – but still a lot better than before! I see the nurse next week – so hopefully I’ll find out more about the dosage, and how long I should be on it.
I’m hoping for miracles over the next few weeks from Isotretinoin! Fingers crossed.
Post publishing edit: This was originally posted on the 2nd April. I had my first clear face on the 5th June. There are still some red marks from previous spots, but otherwise it’s clear! I know this might not be the end, but it’s a pretty major thing to have no spots for the first time in years. I still have a few weeks left on the treatment.
Have you experienced acne as an adult? Which treatments worked for you?
My mum saw the Back Nodger on This Morning a few days ago, and told me about it. The cheapest I found it for was £22.50 on Amazon compared to the £29.99 most places had it available for. I thought it looked interesting, so purchased it.
The Nodger in its packaging.
It arrived today and looks… different to most other massagers! It works by targeting trigger points and allows you to put focused pressure on it. I suffer greatly from very painful trigger points, particularly in my neck, shoulders and lower back.
You push the curved side into your trigger point using the handle. It has a ‘Locator Spot’ which digs into the muscle.
I’ve spent some time trying it out in various tight knots. It works best on my neck, where it’s easier to move around to get the right angle. Similarly, it also does a very good job on my upper back/back of my shoulder blades, and it worked on my arms – but was much more painful than other areas. I didn’t find it at all helpful on my lower back, so I’ll stick to using a tennis ball there!
The end would be quite nice in my lower back – if only I could reach!
All in all – I’m glad I bought it, as it works better than anything else I’ve tried for my neck – and it’s strangely addicting searching for the next painful spot to work on! It will also work nicely in conjuction with my favourite deep tissue massager by Dr Graeme that I find too strong for my neck, and hard to reach the back of my shoulders.
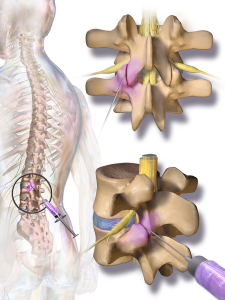
I have pain all over the place, but ranking at the top of the list is my lower back. I’d previously had facet joint injections in my neck and shoulders some years ago, but they didn’t help. However, it was before I’d had an MRI (as it took around 8 years of arguing to get one) and so the consultant was ‘guessing’ at what the issues were. Later on the MRI did clearly show an area in my lower back that had degenerative lumbar disease in the facet joints, arthritis, and others issues. It made a much better target for injections than anywhere else, so I thought it was worth a try.
It took another few years of me arguing for them (nothing ever just seems to just happen on the NHS!) After getting nowhere locally, my Ehlers-Danlos specialist at the Royal National Orthopaedic Hospital at Stanmore sent me to see her Pain Management college, who gave me the go-ahead for bilateral lumbar facet joints at L4/L5 and L5/S1 (so four in total).
A few days passed after being told I could have them and suddenly I thought – what the hell am I doing fighting to have needles put into my spine?! I was sedated during my previous injections, but I did have some memories of the procedure. I remember my consciousness kind of returning and thinking ‘please stop now.’ I was later told the sedation didn’t actually knock you out, but simply wiped your memory – and that you would be aware of what was happening as they did it. This memory built up in my mind until I was convinced I’d be strapped down with horrible painful injections into the middle of my spine, then I’d just forget afterwards so I didn’t realise how awful it would be. So I was about 500 times more nervous for these injections than previously.
The whole topic became a ‘do not discuss’ subject. As soon as I thought about it I went into a state of panic, so there was no research done as I normally would, and I didn’t even allow my mum (who accompanied me) to talk about our arrangements of getting there until the day before. I just wanted to block it totally from my mind.
We travelled to Stanmore the day before for two reasons. The first that I can’t make the journey there and back in one day, and the second was that my admission time was 7am. Ugh!
Although I wasn’t having general anaesthetic, I was told not eat after midnight, and no drinking after 6am. It was the latter I’d struggle with as I’m constantly thirsty.
I arrived at the hospital a couple of minutes before 7am and had a choice of parking for the first time ever! When we reached admissions there were a few people waiting outside, but when the queue got the doorway I realised the room was packed with both people queuing, and waiting in the chairs. It wasn’t the easiest getting my wheelchair in and out with no room for manoeuvring. There was only one member of staff dealing with everyone. The older lady in front of me didn’t speak any English, and was soon joined by an interpreter. The staff member made a phone call and I heard him say, “Are the wards still closed, there are a lot of patients here?” He then informed the interpreter they had a bit of a wait ahead. I was next, and was told the same thing.
I was a little cross, only because getting somewhere for 7am isn’t very easy for me and more importantly 7am = grumpiness! I did later found out the wards were opening for the first time after being closed for two weeks over Christmas – so I assume the delay isn’t normal.
I reached the ward and was met with a number of friendly nurses and health care assistants who welcomed me, and showed me my bed. The lady with the interpreter was in the bed opposite me. A nurse admitted me with a huge pile of paperwork, most of which seemed irrelevant in my case! I was asked a couple of times if I had any allergies. She then took swabs for MRSA and then took my blood pressure (which I hate, as it’s very painful. The muscles in my upper arm are very tight and particularly sensitive). I was told I was third in the queue – and the doctor would be seeing me beforehand.
A couple of other patients got in the bed and went to sleep, which seemed like a good idea – and would also make the time pass. However every time I was about to drift off I was woken by someone. The first to measure me for pressure stockings, then again to tell me I didn’t need them. Then a doctor who was working with my consultant arrived to explain the procedure. I was glad it was her and not my consultant as she was much warmer than my consultant is, which helped. She spent a lot of time explaining how much time they took to sterilise everything to reduce any chance of infection. I wanted to rudely interrupt and say that at that point, I didn’t care – I just wanted her to promise she’d knock me out! She then went through the possible risks – infection, numbness in the legs, pain flaring up afterwards and in a very tiny amount of cases nerve damage. She asked if I had any allergies.
Finally I could ask the one thing I wanted to know.
“You will be sedating me, right?”
“Did you ask for it before?”
“Yes,” I emphasised.
“Then we will.”
“Will I know what’s happening?”
“Well, some people do sleep.”
“Please make that happen with me. Please.”
Then the pharmacist came to take note of my list of medications, and asked whether I had any allergies, then a number of nurses came to tell me, “It won’t be much longer.” Then that they were on their way for me, only to still be there sometime later!
Eventually the porters did arrive and wheeled me into theatre. A nurse went through the final questions – checking I knew what procedure I was having, if I’d had any before, if I had any allergies and if it was definitely my signature on the consent form. The nice doctor then fitted the cannula into my hand, before I lay down front-first on the table. They put an oxygen mask on me, a clip onto my finger to measure oxygen (I’m sure that has a proper name) then to my annoyance – a blood pressure cuff which I was told would be taking my blood pressure every few minutes. It took it twice, before I told the nurse how painful it was. “No problem,” she told me cheerfully, and moved it onto my leg instead which was much better. She then began chatting to me about my hobbies and jewellery making, before my consultant began putting the sanitising fluids on my back. The nice doctor then began to input two injections of sedation into the cannula. I closed my eyes – trying to relax. She then asked if I could still hear her, and I said yes. She thought I’d gone to sleep, and I said I hadn’t felt any sedation yet. She said she’d keep going, and added two more tubes.
The next thing I remember is feeling a bit of pain in my back, and a nurse telling me it was all over. I definitely hadn’t been aware of it. I was taken into recovery for awhile, still very sleepy and groggy. A nurse chatted to me for awhile, and I remember telling her to say thank you to the nurses, as they’d calmed me down a lot beforehand. She promised she would. She then asked if I knew which ward I’d been in.
“It began with J…” I answered.
“Jackson Burrows is the only ward beginning with J.”
“No, it wasn’t that. Was it Diane something?”
“I guess now wasn’t the best time to test your memory?” she laughed. She then came back and said that unfortunately they’d moved me to Margaret Harte Ward. I began to worry if anyone had told my mum as I knew she was planning on getting a cup of tea while I was in the theatre (as she’d very kindly not eaten/drunk anything in front of me while I couldn’t).
As the porters wheeled me out of recovery, the nurse suddenly called for them to stop. She dug through a cupboard, and pulled out another blanket to put around me. “Sorry,” she said to the porters. “I just didn’t want her to get cold on the way back.”
When we got back to the ward I spotted my mum very quickly and realised it was the ward I’d been in all along! The nurse handed over to the ward nurse, and said that my blood pressure had risen quite a bit during the procedure, so they needed to keep an eye on it. Argh, more blood pressure checks!
I was left to sleep for a bit as I slowly came round. A nurse then came round to do the blood pressure test. I admit I groaned, and said the test was hurting quite a bit, then of course after gritting my teeth the machine malfunctioned. Just one more time, I was told. Luckily it was back to normal, and as she took the cuff off she realised lots of red marks had come up all the way round (which are still there today!). She gave me an apologetic pat. I asked if she could take my cannula out as it was pulling quite a bit. She took a look and said it was quite red, and that someone would do it before I left. (Well, one would hope so!)
I was told to stay until lunch time, and then I would be discharged. The nice nurse who admitted me then walked past and so I asked her about the cannula, and she said no problem and took it out. She also checked my ‘wounds’ (just slightly larger than needle marks) and said she was happy with how they looked.
Still waiting opposite me was the older lady with the interpreter. I heard a nurse say to her that her operation wasn’t going to be until mid-afternoon – yet she’d been admitted at 7am! It seemed mean to make her wait so long, and I assume the NHS had paid extra for the interpreter when they could had admitted her at the 11am or 2pm admission times. I noticed the little old lady chatted non-stop to her interpreter, which made me smile as I could just imagine in the 7+ hours the interpreter sat with her she got to hear her entire life story.
I left at 1:40pm, slept all the way home, slept all afternoon and very unusually for me – all night!
So all in all – it wasn’t nearly as bad as I dreaded. The staff – particularly the nurses, were lovely. There were lots of touches of kindness, like the nurse in the theatre distracting me from my nerves, the recovery nurse chatting to me as I came round and making sure I was warm, and the staff back on the ward who took care of me and offered me toast and regular drinks when I came round. They all made it a much easier experience. Also – the NHS really, really want to know if you have any allergies.
I’m in a lot of pain now which feels different to my usual pain. I was warned I may flare up, particularly where the needle touches the bone – so I’ve no idea if it worked yet. I think I need to wait for all of that to calm down over the next couple of days before I can tell if it helped.