by The Chronic Chronicles | Jan 26, 2014 | Access, Wheelchair
In the next year some of you may be pondering the decision of whether or not to use a wheelchair, if you’re finding walking painful or exhausting.
It’s an incredibly difficult decision, and there are often a few reasons why this hesitation happens. For some it can feel like giving in, that’s you’ve stopped fighting. It can sometimes feel like you’re sacrificing your mobility – that if you have a wheelchair you won’t push yourself walk at all anymore. There can be a stereotype that wheelchairs are for people who cannot walk at all, or just for older people. It can feel embarrassing, or like you’re making a big deal out of your situation. There are lots of valid (and some not so valid) reasons that can make that step a hard one.
The main suggestion I put to people wrestling with this decision is – are you avoiding going to places because you struggle to walk around? Have you stopped going out for a walk with your family, going on a shopping trip or not even considering an evening out with friends?
That’s the position I found myself in a few years ago. I was simply avoiding those activities because walking was so painful. One day someone offered to push me around a supermarket in a manual wheelchair they had available for customers. I hesitated – they were for people with disabilities! Eventually I gave it a go, and the difference it made was incredible. I could spend time looking at what I wanted, browsing through the aisles – something I hadn’t been able to do for a long time. My attitude changed, and I began visiting shops or places I knew had wheelchairs or scooters for customer use. (I also accepted I was one of those people with disabilities during this time.)
I did find being pushed in a manual wheelchair very odd though, but it was my only choice as I’m unable to self-propel. It feels like you’re giving all of your independence over to the person pushing you, and it’s hard to explain what this feels like – as an adult who has been making their own decisions for years. That person has the power to decide where you go and what you will do, and you have to trust them implicitly. It’s also a physically exhausting job for them. There are lots hazards you don’t really consider when walking such as hills, pot holes and curbs, plus generally poor accessibility like having no ramps, tight turns, advertising boards on the pavements and other street furniture. The strain it put on the person pushing made me feel very guilty.
The cost of a wheelchair or scooter can also be difficult to afford. I was provided a manual wheelchair on the NHS, but as I couldn’t use it independently and didn’t have anyone to push me around 24/7, it mostly sat gathering dust. The decision for upgrading the manual was taken out of my hands by damage to my spine that means I can now only walk very short distances. As I was working at the time I was able to apply for grant funding for an electric wheelchair and a hoist for my car that was available to help disabled people in employment. Other options include schemes to lend a chair or scooter for a short period of time, charitable grants or medical insurance that may help towards a purchase. A decent wheelchair will be costly, but it’s also worth considering buying second-hand through private sellers or online outlets.
However, getting a wheelchair changed my world overnight. I’ve been able to go on family outings, visit local parks and enjoy trips out to local shops. It means I can save my energy and pain levels from increasing through walking and use them on enjoying myself instead. I still sometimes feel awkward around family and people I haven’t seen in awhile – but if they can’t accept your need to get around without agonising pain – that’s their problem.
So if you’re sitting at home still trying to make that decision and thinking of the negatives – try to think of all the positive things you could do that you haven’t been able to do in some time if you’ve struggled with walking. A wheelchair could open more of the world to you.
My wheelchair – an Invacare TDX

by The Chronic Chronicles | Jan 22, 2014 | Benefits, Opinion
Yesterday I had an assessment by Social Services for Direct Payments. I’d been waiting about seven months for it after being assessed as ‘Urgent’. The Social Worker was fine – we talked through my condition, how it impacts me, the average day and what help I need.
What I did find interesting during the assessment is that after I was asked to give an overall idea of the help I’d ideally like – she then gave me a list of everything that my Disability Living Allowance was expected to cover, and so Social Services would not. From my list this included all cleaning, gardening, treatments not covered by the NHS, help with pets, and any activities even if they related to quality of life/better health and more.
As an aside, while I was aware of the cleaning issue, I am appalled that Social Services won’t help people with disabilities with cleaning at all. It’s not a cheap service to have, and I find it totally impossible to do such physical tasks as hovering, dusting, clothes washing, changing the bed sheets – and there’s people a lot worse than me out there. So they’ll pay to get you out of bed, and showered – then leave you in squalor to fend for yourselves?
But, back to my main point, I thought it was interesting how far she expected DLA to stretch. I currently use my DLA for an adapted car that has a hoist for my wheelchair. Without this, I couldn’t leave the house – as my wheelchair won’t go on buses, and wheelchair-adapted taxis are a rare sight to behold in my town (and usually double the price). Other people will often use this payment to hire a wheelchair from Mutability, or on taxis to get out and about.
Out of the rest of my DLA I and many others pay for things like extra heating, carers, mobility aids, therapeutic devices, special clothing/shoes, food that’s easier to cook (pre-prepared), the higher rents of accessible accommodation, medications, supplements, extra washing loads, specialist exercise programmes, special cushions, adapted items, insurance for wheelchair/scooter, petrol for additional car journeys (doctors/hospitals/travel to specialists often miles away, physiotherapists, other therapists, assessments as well as journeys most people would walk – but you have to drive instead) and so much more.
Of course people with disabilities are statistically more likely to be on a lower-income than the average person, even when able to work. So DLA may also help towards rent, bills and normal day-to-day living costs.
When I was trying to obtain an electric wheelchair through the NHS, as I am physically unable to manually propel – I explained I was using my Mobility Payments on a car that I needed to get to work. The assessors response was that I should be using it on a wheelchair. I pointed out that if I used it on a wheelchair and gave up my car, the wheelchair would have to live in the garden – and I would have to live on the sofa, as the car was vital in transporting the wheelchair, so what would be the point of that? She had no answer. It seemed it was their policy to be telling people to spend the DLA on wheelchairs too.
But it doesn’t cover a fraction of the extra costs I have for being disabled, and while I totally understand there isn’t a limitless supply of funds – it doesn’t help when agencies are putting more and more strain onto the benefit. Exactly how far do they expect DLA to go?

by The Chronic Chronicles | Jan 16, 2014 | Reviews, Treatment
My mum saw the Back Nodger on This Morning a few days ago, and told me about it. The cheapest I found it for was £22.50 on Amazon compared to the £29.99 most places had it available for. I thought it looked interesting, so purchased it.
The Nodger in its packaging.
It arrived today and looks… different to most other massagers! It works by targeting trigger points and allows you to put focused pressure on it. I suffer greatly from very painful trigger points, particularly in my neck, shoulders and lower back.

You push the curved side into your trigger point using the handle. It has a ‘Locator Spot’ which digs into the muscle.
I’ve spent some time trying it out in various tight knots. It works best on my neck, where it’s easier to move around to get the right angle. Similarly, it also does a very good job on my upper back/back of my shoulder blades, and it worked on my arms – but was much more painful than other areas. I didn’t find it at all helpful on my lower back, so I’ll stick to using a tennis ball there!

The end would be quite nice in my lower back – if only I could reach!
All in all – I’m glad I bought it, as it works better than anything else I’ve tried for my neck – and it’s strangely addicting searching for the next painful spot to work on! It will also work nicely in conjuction with my favourite deep tissue massager by Dr Graeme that I find too strong for my neck, and hard to reach the back of my shoulders.
by The Chronic Chronicles | Jan 8, 2014 | Hospitals, Treatment
I have pain all over the place, but ranking at the top of the list is my lower back. I’d previously had facet joint injections in my neck and shoulders some years ago, but they didn’t help. However, it was before I’d had an MRI (as it took around 8 years of arguing to get one) and so the consultant was ‘guessing’ at what the issues were. Later on the MRI did clearly show an area in my lower back that had degenerative lumbar disease in the facet joints, arthritis, and others issues. It made a much better target for injections than anywhere else, so I thought it was worth a try.
It took another few years of me arguing for them (nothing ever just seems to just happen on the NHS!) After getting nowhere locally, my Ehlers-Danlos specialist at the Royal National Orthopaedic Hospital at Stanmore sent me to see her Pain Management college, who gave me the go-ahead for bilateral lumbar facet joints at L4/L5 and L5/S1 (so four in total).
A few days passed after being told I could have them and suddenly I thought – what the hell am I doing fighting to have needles put into my spine?! I was sedated during my previous injections, but I did have some memories of the procedure. I remember my consciousness kind of returning and thinking ‘please stop now.’ I was later told the sedation didn’t actually knock you out, but simply wiped your memory – and that you would be aware of what was happening as they did it. This memory built up in my mind until I was convinced I’d be strapped down with horrible painful injections into the middle of my spine, then I’d just forget afterwards so I didn’t realise how awful it would be. So I was about 500 times more nervous for these injections than previously.
The whole topic became a ‘do not discuss’ subject. As soon as I thought about it I went into a state of panic, so there was no research done as I normally would, and I didn’t even allow my mum (who accompanied me) to talk about our arrangements of getting there until the day before. I just wanted to block it totally from my mind.
We travelled to Stanmore the day before for two reasons. The first that I can’t make the journey there and back in one day, and the second was that my admission time was 7am. Ugh!
Although I wasn’t having general anaesthetic, I was told not eat after midnight, and no drinking after 6am. It was the latter I’d struggle with as I’m constantly thirsty.
I arrived at the hospital a couple of minutes before 7am and had a choice of parking for the first time ever! When we reached admissions there were a few people waiting outside, but when the queue got the doorway I realised the room was packed with both people queuing, and waiting in the chairs. It wasn’t the easiest getting my wheelchair in and out with no room for manoeuvring. There was only one member of staff dealing with everyone. The older lady in front of me didn’t speak any English, and was soon joined by an interpreter. The staff member made a phone call and I heard him say, “Are the wards still closed, there are a lot of patients here?” He then informed the interpreter they had a bit of a wait ahead. I was next, and was told the same thing.
I was a little cross, only because getting somewhere for 7am isn’t very easy for me and more importantly 7am = grumpiness! I did later found out the wards were opening for the first time after being closed for two weeks over Christmas – so I assume the delay isn’t normal.
I reached the ward and was met with a number of friendly nurses and health care assistants who welcomed me, and showed me my bed. The lady with the interpreter was in the bed opposite me. A nurse admitted me with a huge pile of paperwork, most of which seemed irrelevant in my case! I was asked a couple of times if I had any allergies. She then took swabs for MRSA and then took my blood pressure (which I hate, as it’s very painful. The muscles in my upper arm are very tight and particularly sensitive). I was told I was third in the queue – and the doctor would be seeing me beforehand.
A couple of other patients got in the bed and went to sleep, which seemed like a good idea – and would also make the time pass. However every time I was about to drift off I was woken by someone. The first to measure me for pressure stockings, then again to tell me I didn’t need them. Then a doctor who was working with my consultant arrived to explain the procedure. I was glad it was her and not my consultant as she was much warmer than my consultant is, which helped. She spent a lot of time explaining how much time they took to sterilise everything to reduce any chance of infection. I wanted to rudely interrupt and say that at that point, I didn’t care – I just wanted her to promise she’d knock me out! She then went through the possible risks – infection, numbness in the legs, pain flaring up afterwards and in a very tiny amount of cases nerve damage. She asked if I had any allergies.
Finally I could ask the one thing I wanted to know.
“You will be sedating me, right?”
“Did you ask for it before?”
“Yes,” I emphasised.
“Then we will.”
“Will I know what’s happening?”
“Well, some people do sleep.”
“Please make that happen with me. Please.”
Then the pharmacist came to take note of my list of medications, and asked whether I had any allergies, then a number of nurses came to tell me, “It won’t be much longer.” Then that they were on their way for me, only to still be there sometime later!
Eventually the porters did arrive and wheeled me into theatre. A nurse went through the final questions – checking I knew what procedure I was having, if I’d had any before, if I had any allergies and if it was definitely my signature on the consent form. The nice doctor then fitted the cannula into my hand, before I lay down front-first on the table. They put an oxygen mask on me, a clip onto my finger to measure oxygen (I’m sure that has a proper name) then to my annoyance – a blood pressure cuff which I was told would be taking my blood pressure every few minutes. It took it twice, before I told the nurse how painful it was. “No problem,” she told me cheerfully, and moved it onto my leg instead which was much better. She then began chatting to me about my hobbies and jewellery making, before my consultant began putting the sanitising fluids on my back. The nice doctor then began to input two injections of sedation into the cannula. I closed my eyes – trying to relax. She then asked if I could still hear her, and I said yes. She thought I’d gone to sleep, and I said I hadn’t felt any sedation yet. She said she’d keep going, and added two more tubes.
The next thing I remember is feeling a bit of pain in my back, and a nurse telling me it was all over. I definitely hadn’t been aware of it. I was taken into recovery for awhile, still very sleepy and groggy. A nurse chatted to me for awhile, and I remember telling her to say thank you to the nurses, as they’d calmed me down a lot beforehand. She promised she would. She then asked if I knew which ward I’d been in.
“It began with J…” I answered.
“Jackson Burrows is the only ward beginning with J.”
“No, it wasn’t that. Was it Diane something?”
“I guess now wasn’t the best time to test your memory?” she laughed. She then came back and said that unfortunately they’d moved me to Margaret Harte Ward. I began to worry if anyone had told my mum as I knew she was planning on getting a cup of tea while I was in the theatre (as she’d very kindly not eaten/drunk anything in front of me while I couldn’t).
As the porters wheeled me out of recovery, the nurse suddenly called for them to stop. She dug through a cupboard, and pulled out another blanket to put around me. “Sorry,” she said to the porters. “I just didn’t want her to get cold on the way back.”
When we got back to the ward I spotted my mum very quickly and realised it was the ward I’d been in all along! The nurse handed over to the ward nurse, and said that my blood pressure had risen quite a bit during the procedure, so they needed to keep an eye on it. Argh, more blood pressure checks!
I was left to sleep for a bit as I slowly came round. A nurse then came round to do the blood pressure test. I admit I groaned, and said the test was hurting quite a bit, then of course after gritting my teeth the machine malfunctioned. Just one more time, I was told. Luckily it was back to normal, and as she took the cuff off she realised lots of red marks had come up all the way round (which are still there today!). She gave me an apologetic pat. I asked if she could take my cannula out as it was pulling quite a bit. She took a look and said it was quite red, and that someone would do it before I left. (Well, one would hope so!)
I was told to stay until lunch time, and then I would be discharged. The nice nurse who admitted me then walked past and so I asked her about the cannula, and she said no problem and took it out. She also checked my ‘wounds’ (just slightly larger than needle marks) and said she was happy with how they looked.
Still waiting opposite me was the older lady with the interpreter. I heard a nurse say to her that her operation wasn’t going to be until mid-afternoon – yet she’d been admitted at 7am! It seemed mean to make her wait so long, and I assume the NHS had paid extra for the interpreter when they could had admitted her at the 11am or 2pm admission times. I noticed the little old lady chatted non-stop to her interpreter, which made me smile as I could just imagine in the 7+ hours the interpreter sat with her she got to hear her entire life story.
I left at 1:40pm, slept all the way home, slept all afternoon and very unusually for me – all night!
So all in all – it wasn’t nearly as bad as I dreaded. The staff – particularly the nurses, were lovely. There were lots of touches of kindness, like the nurse in the theatre distracting me from my nerves, the recovery nurse chatting to me as I came round and making sure I was warm, and the staff back on the ward who took care of me and offered me toast and regular drinks when I came round. They all made it a much easier experience. Also – the NHS really, really want to know if you have any allergies.
I’m in a lot of pain now which feels different to my usual pain. I was warned I may flare up, particularly where the needle touches the bone – so I’ve no idea if it worked yet. I think I need to wait for all of that to calm down over the next couple of days before I can tell if it helped.
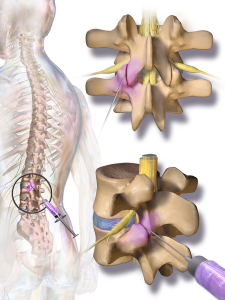
An image of a facet joint injection

by The Chronic Chronicles | Jan 1, 2014 | Daily Life
A New Year generally brings about mixed feelings. Traditionally it’s a time to reflect over the year that’s passed, the good and the bad – and also to think about your aspirations for the year ahead. It’s also a chance to draw a line under the negative, and to have a fresh start.
Over the last few years those goals for the year ahead have shifted quite dramatically for me. They used to be around completing my studies, and then became quite work focused – whether it was finding a job I loved, or making progress within my work. Taking the project I was working on forward, or becoming a manager. They may have also been more fun – like sharing memories with friends, going on holiday with family, or visiting new places.
Over the Christmas period I managed to meet up with friends I hadn’t seen in awhile, and family members who told me their news, and it’s been playing on my mind ever since. They’re just getting on with their lives – getting engaged, celebrating promotions at work, looking forward to their holidays abroad, planning on meeting up for weekly squash. The kind of normality that’s just faded away for me. Thinking about the things that stick out for me from 2013 – they’re sadly mostly health focused, like being given the go-ahead for some new treatments, the nice consultants I saw, and the nasty ones. And then the biggest – having to stop working.
When I look forward into 2014 I see a couple of dates – the lumbar injections in January, the infusions in March. Then a whole lot of nothingness. I don’t know what will happen in 2014. Obviously no one does, unless they have a handy crystal ball – but every year since I was 15, my physical health has been quite rapidly declining. Each year I can cross a few more things off the list I can no longer do. This time last year I was just about holding a job down, this year I’ve spent more of my week in bed, than functioning.
Even New Year’s Eve itself was quite different this year. Having had a bad night previously, I spent most of the day asleep. I woke at 6pm, and it took awhile for me to even realise it was New Year’s Eve!
That said – if I continued to dwell on what’s changed or will continue to, or if I thought “well there isn’t any point anymore!” then nothing will improve. Instead it’s about shifting priorities – finding interests and hobbies that are manageable, and allow me to have things to look forward to without feeling like life has hit stalemate. Or even better, saying to myself, “I’ve survived another year. It wasn’t easy, it was painful – but I’ve done it, and can continue to do it.”
But if you are someone who is able to go to weekly ‘insert activity of choice’, head out for a drink with friends at the last minute, or can go on holiday and spend all your time planning what you’ll do when you get there – then treasure it. Please. Health is precious – and can vanish in an instant.

by The Chronic Chronicles | Dec 23, 2013 | Hospitals
I stumbled across the treatment of ‘infusions’ sometime ago, and then kept seeing them being mentioned. I began to try to find out more about them, but information was limited.
I was aware it usually consisted of either Ketamine or Lidocaine being given by an IV, and for some it works really well for pain relief. For others it seems to do nothing at all.
Eventually a friend kindly offered to search the academic databases he had access to and sent me all the research he could find. They were generally all positive.
‘Intravenous Lidocaine: An Outdated or Underutilized Treatment for Pain?’ by Gary McCleane stated, “The drug is administered over a relatively short period of time and yet the potential relief lasts significantly beyond both the period of administration and the plasma half-life of this local anesthetic.” He goes on to state that, “an infusion over a few hours can produce relief that extends to weeks and even months. Consequently, side effects, if any are apparent, are short lived and last for a much shorter time than the pain relief.”
McCleane explained that for many patients undertaking this treatment it becomes their only form of pain-relief, and they’re able to stop all other medications for pain. A trial of 82 patients found that 82% had a very good pain reduction after their infusion. In a second study on people with Fibromyalgia it was found that 40% of patients had between 13-18 weeks of relief.
A second study called ‘Efficacy and adverse effects of intravenous lignocaine therapy in fibromyalgia syndrome’ concluded that the therapy “appears to be both safe and of benefit in improving pain and quality of life for patients with fibromyalgia.”
The one downside is that there wasn’t much research on the therapy, and when a study had taken place they had very small sample sizes. There are also side effects such as hypotension, tachycardia, infections and other such fun times.
I began by asking my GP about them, but she’d never heard of them. I asked at the various London hospitals I’m under, but was told they didn’t do them. I came across a number of people with Ehlers-Danlos Syndrome who’d had them, but it was never at a hospital near to me.
I then visited a pain clinic in another town but they too stated they didn’t do them, and if they did they wouldn’t do it for Ehlers-Danlos Syndrome as there weren’t enough of us with it. (Red flag to a bull!)
I then changed GPs, and she too hadn’t heard of them – but a few weeks later I got a phone call from her. She explained she’d just had a patient in to see her who’d just had infusions at the hospital in my own town! She told me to come and see her, and she’d get me referred.
I saw a consultant at the pain clinic last week and she agreed I could have one infusion. I’m not sure why just one, but still it’s good news!
I’m also due to have facet joint injections in January, so there are two treatments coming up that allow me to have some hope.
An IV
Credit to: andyk

by The Chronic Chronicles | Dec 16, 2013 | Coping Methods
When you’re in constant pain, it’s very easy to focus on it. It can become all-consuming, and the more you think about it – the worse it feels. Someone once suggested to me that I try crafting as a means of distraction. I have to be honest, I was a little annoyed – how would painting a pretty picture take my crippling pain away? It seemed a little dismissive. Plus there was also the fact I’d never thought of myself as a particularly creative or artistic person. At school even my doodled stick figures ran screaming in terror, and my art teacher made it clear it wasn’t my forte, but I thought I’d give card-making a try.
I enjoyed making them, but they weren’t that great. I’d look online at all the beautiful designs people were creating, and it just didn’t feel quite like me. After I’d spent a fortune on card-making supplies, I decided to try my hand at jewellery instead, and in doing so found a new passion.
Stargazer Watch
The early days of making jewellery weren’t easy – my hands cramped up terribly, and I was left with blisters all over my skin. In time my dexterity improved and it helped strengthen some of my muscles in my hands. And it was true – when I’m busy concentrating on making a new item, my brain is focused elsewhere. It doesn’t make the pain go away, it just redirects my attention so I’m not thinking about it, which is really helpful.
Once I joined the world of crafting – I found more and more other people with disabilities were also there, and finding an outlet in art – by painting, woodwork, ceramics, photography or anything in-between. For example a friend of mine makes ‘pain monsters’ from felt when she’s having a bad day, which helps her create a visual representation of what she’s feeling.
It took me quite a long time to find out what was wrong with me. Many years of fighting and pleading with the medical community to stop shrugging their shoulders, and to do something. When I was told I had Fibromyalgia, it came as something of a relief. I felt like I wasn’t alone – there were other people with this stupidly long list of symptoms out there. I wanted to commemorate the end of that fight, that also informed people about the condition. I made my first Fibromyalgia awareness bracelet not long after, and then began to receive requests to create ones for other conditions – including some I’d never heard of before. People liked the more personalised feel to the more generic rubber bands that are usually sold. My biggest seller was for Marie Charcot Tooth Disease, and eventually the national charity began to order from me so they could sell them on their website.
I also auctioned lots of my bracelets off for the Fibromyalgia Association UK, and also for Ehlers-Danlos Syndrome related charities when I was diagnosed, a genetic multi-systemic connective tissue disorder. It made me feel like I was helping, even in one tiny way.

An Ehlers-Danlos Syndrome bracelet featuring zebra stripe beads – the symbol of the condition
It’s very common to walk into a shop and see a row of pink coloured items for Breast Cancer awareness. Yet there are so many other conditions that people often haven’t even heard of before, let alone understand what they entail and what it’s like to live with them. People have often told me when wearing one of my awareness bracelets it has sparked conversations with friends and family who had never asked about their health before.

Fibromyalgia Awareness Bracelet

Fibromyalgia Awareness Bracelet 2
The colours of the bracelets are usually picked by the existing awareness ribbon colour, and if there isn’t one, then by the colours of the national organisation/charity for the condition. Sometimes there are obvious symbols that can be included as charms. Fibromyalgia often has an association with butterflies, Autism with jigsaw pieces, Charcot Marie Tooth Disease with hands and feet. Sometimes a spoon charm is added from the fantastic analogy “The Spoon Theory” by Christine Miserandino, to which many people with chronic illness resonated with. My most commonly used charm is simply a silver ribbon with the word hope written on it – as I believe that’s something we all need in some form or another.

Arthritis Awareness Bracelet
In April this year I had to stop working due to my health continuing to get worse. Being able to make jewellery – even if it’s for twenty minutes in the middle of the night when I’m struggling to sleep, has helped keep my spirits up and creativity flowing.
If you’re interested in seeing more of my jewellery and awareness items you can find me under Sparkly Place Jewellery on Facebook.

by The Chronic Chronicles | Dec 14, 2013 | Benefits
This year my health has gone downhill somewhat. I suppose it has been doing that for some time, but when I finished my previous job I just knew I couldn’t do it anymore. I was a total mess, and my list of needs and adjustments from a job was getting longer than the job description itself.
In April I applied for Employment and Support Allowance for the first time. For those of you that don’t know much about it, it’s the benefit that replaced Incapacity Benefit – for disabled people who can no longer work.
There are three rates – the Assessment Rate, the Work Related Activity Group (WRAG) and the Support Group. If placed in the WRAG they admit you’re too ill to work currently, but feel you should be able to work with support in the future. People in this group have to attend regular work-related meetings with companies who receive bonuses if they can get you into work; can be forced into unlimited work-placements and can even sanction you. So in one breath they admit people in this group cannot work, and then force them too – and stop their benefits if they refuse. The Support Group means they feel you cannot work, and do not expect you to anytime soon.
The way the system is supposed to work is that you receive the assessment rate for 13 weeks, then either a decision maker at the Department of Work and Pensions (DWP) decides if you should go in a group or be found ‘fit for work.’ If they feel they don’t have enough information they can send you for a medical with ATOS. The assessment rate is lasting much longer than 13 weeks, however, which is probably because a large amount of people are being sent for the medicals despite copious medical evidence with their applications that should give the decision maker enough information to decide.
The medical tests themselves are highly controversial as it’s been shown those carrying them out are under a lot of pressure to find the person fit for work. The tests are extremely limited in scope, and most people are indeed found fit for work and then have to appeal it. In most cases this decision is overturned at tribunal level – showing the system is flawed. The whole process causes a lot of stress to the claimant and this horror vastly increased in October when they decided that if you were found fit for work and appealed, you’d no longer be paid the assessment rate while you waited for the tribunal – which can take up to a year to happen. The benefit starts at £56.80 a week for under 25s, and £71.70 for over 25s. This amount is what people have to live on, and removing it is beyond cruel.
In July I was told I would be having a medical. While expecting this, I was still annoyed as my claim included excellent medical evidence. My GP had written a long letter, as well as my Occupational Therapist. I also had a pile of letters from my consultants including the top specialist in Ehlers-Danlos Syndrome in Britain.
But I heard nothing for six months. When October passed my worry increased dramatically. I wondered what would happen if I was found fit for work and had no income while I appealed. I fretted about how I’d pay the rent for the accessible bungalow I live in, or pay for the treatment the NHS won’t cover.
I’ve also been through all this before with Disability Living Allowance and it wasn’t a very fun time. I pretty much had a mini-break down and had to go through two tribunals. You can read about that starting here and follow the whole saga under the tag ‘benefit claim’.
Having had bad news so often before, and living in constant fear of bad news from the DWP – I have a certain reaction every time I spot their distinctive letter I call the ‘dreaded brown envelope.’
I’m a little superstitious, even though I know it’s silly. I say the rhyme when I see a lone magpie, I throw spilt salt over my shoulder and I make a wish when the numbers on a clock are all the same. I’d been lying awake for some hours trying to sleep (not uncommon) when I spotted it was 2:22am. I made a wish. “Please. Please just let me know either way before Christmas.”
The next morning I was hobbling past the front door when it caught my eye. The dreaded brown envelope. My heart began to thump and my breath caught in my throat. I opened it quickly, and tried to make sense of it. Two words stood out to me – Support Group.
Relief flared through me, but as I read further it stated that I’d been placed in the Support Group from July – 30th November.
When you get put in a group a time of claim goes along with it, and I was aware that people have been placed in a group before and thought they were okay, only to find out that by the time they’d been told which group they were in, their claim had finished. Was that what had happened to me?
I immediately phoned the DWP and spoke to a nice lady who looked my claim up, and agreed that the letters were confusing, but those dates were referring to back pay. They agreed I should have gone into the Support Group from July, and up until November 30th had been on the assessment rate. So I’d get back pay up of the difference between the Assessment Rate and Support Group Rate until that date. Then from the 30th November my claim will run for two years.
I began to cry – and apologised to the poor woman. I explained I was just so relieved. She responded kindly by saying I didn’t have to worry about any medicals, or sending anymore sick notes.
I honestly can’t believe I got put into the Support Group first time and didn’t have to go through a medical. It seems incredibly rare with ESA not to have a medical, and even more so to be put straight into the Support Group.
I can’t even begin to put into words what this means to me. It should mean some financial stability during this time – until the Personal Independence Payments rollout.
Credit to: Cieleke

by The Chronic Chronicles | Nov 6, 2013 | Benefits
A person with a disability has won a case against housing benefits officials when a judge ruled that a reduction of her housing benefit breached her human rights. It was agreed that she does require a separate room from her husband due to the her MS and the adaptations she required.
This has positive implications for all of those with a disability impacted by the tax. Currently disabled people make up 63% of all those receiving a reduction in their housing benefit due to having a ‘spare bedroom’.
In fact the bedroom is rarely spare – it’s often used to store medical equipment, been adapted for a specific purpose, used for those who can’t sleep in the same room as someone else due to their condition, or for someone who requires a carer – but not every night.
The worst part of the new scheme penalising so many people is there isn’t a choice in the matter. One and two bedroom properties simply aren’t available, let alone houses that are suitably adapted. Often the person with a disability or the council have spent thousands of pounds on putting the right adaptations in place, sometimes even building an extension if the property wasn’t large enough to meet their needs. It’s then a cruel irony the room provided to make life easier for them ends up reducing their already inadequate benefits.
The Papworth Trust have reported that disabled people being hit by the tax are being forced to cut back essentials such as food and other bills, and they state this “will also have a longer term impact on the NHS and social services.”
While Labour have now promised to scrap the bedroom tax if they get into power, this cruel policy should be halted immediately to stop penalising the 420,000 disabled people impacted by this policy, and further 240,000 people on a low-income.
Credit to Jason Morrison at http://www.creationcafe.com

by The Chronic Chronicles | Oct 22, 2013 | General Posts
Living Well with Fibromyalgia is an online magazine written by and for people with the condition, and published by the fabulous website FibroModem. They are currently looking for people who would like to appear on the cover. It’s a great way to represent the normal people living with the condition, as well as get your chance to be a star!
You need to submit your photo by the 1st November to contributions@fibromodem.com. Full terms and conditions can be found here.
Good luck!

by The Chronic Chronicles | Oct 16, 2013 | Doctors
By 2010 I’d seen a string of consultants over the years, but none had been able to tell me what was wrong. They’d all been appointments of around 15 minutes, a quick look at my spinal movement, a couple of questions , a shrug of their shoulders and a dismissal. I left each appointment feeling lost and disappointed.
A physiotherapist then mentioned I was very hypermobile, which then put me on a path of research into what that meant, the implications and I then came across the condition Ehlers-Danlos Syndrome which seemed to fit all my symptoms. I also found that one of the top specialists in the condition, Professor Rodney Grahame, was based at the University College Hospital London.
I then had quite a fight to get the referral, having to go through the PCT and Rheumatology department at my local hospital – but finally I was informed they were willing to refer me for a second opinion and I had the funding for it.
It took about six months until I saw Professor Grahame, in January 2011. I knew he was different when he began to put together a detailed overview from my birth to the current day. I was with him for over an hour – and he was very thorough and polite. He explained what was wrong with me, and some of the things I could try – including referrals to other specialists. I felt listened to, respected and finally had the answers I had been seeking for so long. He also followed my appointment up with a very detailed report that helped me secure further support from other sources.
I saw him again eighteen months later for a follow-up, where again he was very helpful, and enabled me to have further testing within weeks, that I’d been asking for locally for the past two years.
Sadly, Professor Grahame retired this year and it’s a massive setback for the Ehlers-Danlos Syndrome sufferers in the UK. There is a shocking lack of specialists and clinics in the UK – and Professor Grahame has been unfailing in his research and support. He changed the lives of so many families by finally being able to give answers to people sometimes after decades of uncertainty. He brought a particular kindness and expertise that many others lack.
He will be sorely missed at the UCHL, but I hope he enjoys his retirement!

by The Chronic Chronicles | Oct 11, 2013 | Coping Methods, Daily Life
Frustration. Credit to Staci Becker
I don’t tend to cry. I mean – give me a sad film, or book and I’m sobbing like nobody’s business. But in pain, randomly when it’s all just got too much? Not that often. (Although let’s take my last year of work out of the equation, because dear god I was a mess.)
But I have cried in my last three appointments, and all three times it was around the same topics. Frustration at the “system” and exercise.
The last few months have been tough for me. My condition seems to have gone into haywire, insomnia has struck big time, my pain levels are pretty damn ridonkulous and I’ve been pretty much stuck in the house. It’s always tough when you have a flare up, because of the fear this is your new reality. This is the next downward slide, on a slide that’s been pretty slippery for the last eleven years. At the same time there has to be hope. Sometimes I pin it on myself – I’m going to try this supplement, and do these new stretches eight times a day until every muscle in my body is strengthened and then…
And then I’m doing the most basic of basic stretches, and put my joint out, and I’m lying on the floor with half my body shaking in spasm, trying not to throw up and thinking if I can just make it back to the sofa and not move for five days, it will be okay.
So then I pin that hope on others. That I’m going to go to the physio and they’ll give me as much Hydrotherapy as I need, and then I’ll see the pain consultant and they’ll read the research I’ve found around a specific new medication that looks really promising and will give it to me without a fight, and then…
And then I’m sitting with the physiotherapy who is giving me the lecture that they don’t have infinite resources, so I can have one more block of hydrotherapy next year, and then that’s it. I’ll have to find somewhere else to go, and I’m trying to explain there is nowhere else, nowhere accessible, nowhere affordable, and I’m crying because I just want them to say yes, no problem, for once.
And then I’m at the pain consultant – the one that’s meant to work with people with Ehlers-Danlos Syndrome a lot, except she’s getting the most basic elements of the condition wrong. She does read the research I push at her, and she turns and says – “Yes, we do this here.” There’s a pause, my heart races. “But not for people with your condition.” And then she’s lecturing me – you need to exercise, and push through the pain, it can’t be that bad. And I’m trying to tell her, explain that I’m not talking about aching muscles the next day after a session at the gym, but agonising and consuming pain, partial dislocations – bedbound for days, and I’m crying because she doesn’t get it.
And then I’m at the osteopath, and she has her elbow in my lumbar spine, and she says, “Have you considered exercise?” And I sigh internally, but politely try to explain the same old issues, that I do exercise – but it has to be extremely limited, and she’s pushing it and pushing it until the tears are there again and then she’s backpedalling, and sorry.
It’s so frustrating, I hate crying – and on their own are such minor things. It’s the build up of it all, the feeling they’re just not listening.
But I need to wipe my tears, because it gets me nowhere, and push on with what I can. I’ll get there.