by The Chronic Chronicles | Jan 26, 2014 | Access, Wheelchair
In the next year some of you may be pondering the decision of whether or not to use a wheelchair, if you’re finding walking painful or exhausting.
It’s an incredibly difficult decision, and there are often a few reasons why this hesitation happens. For some it can feel like giving in, that’s you’ve stopped fighting. It can sometimes feel like you’re sacrificing your mobility – that if you have a wheelchair you won’t push yourself walk at all anymore. There can be a stereotype that wheelchairs are for people who cannot walk at all, or just for older people. It can feel embarrassing, or like you’re making a big deal out of your situation. There are lots of valid (and some not so valid) reasons that can make that step a hard one.
The main suggestion I put to people wrestling with this decision is – are you avoiding going to places because you struggle to walk around? Have you stopped going out for a walk with your family, going on a shopping trip or not even considering an evening out with friends?
That’s the position I found myself in a few years ago. I was simply avoiding those activities because walking was so painful. One day someone offered to push me around a supermarket in a manual wheelchair they had available for customers. I hesitated – they were for people with disabilities! Eventually I gave it a go, and the difference it made was incredible. I could spend time looking at what I wanted, browsing through the aisles – something I hadn’t been able to do for a long time. My attitude changed, and I began visiting shops or places I knew had wheelchairs or scooters for customer use. (I also accepted I was one of those people with disabilities during this time.)
I did find being pushed in a manual wheelchair very odd though, but it was my only choice as I’m unable to self-propel. It feels like you’re giving all of your independence over to the person pushing you, and it’s hard to explain what this feels like – as an adult who has been making their own decisions for years. That person has the power to decide where you go and what you will do, and you have to trust them implicitly. It’s also a physically exhausting job for them. There are lots hazards you don’t really consider when walking such as hills, pot holes and curbs, plus generally poor accessibility like having no ramps, tight turns, advertising boards on the pavements and other street furniture. The strain it put on the person pushing made me feel very guilty.
The cost of a wheelchair or scooter can also be difficult to afford. I was provided a manual wheelchair on the NHS, but as I couldn’t use it independently and didn’t have anyone to push me around 24/7, it mostly sat gathering dust. The decision for upgrading the manual was taken out of my hands by damage to my spine that means I can now only walk very short distances. As I was working at the time I was able to apply for grant funding for an electric wheelchair and a hoist for my car that was available to help disabled people in employment. Other options include schemes to lend a chair or scooter for a short period of time, charitable grants or medical insurance that may help towards a purchase. A decent wheelchair will be costly, but it’s also worth considering buying second-hand through private sellers or online outlets.
However, getting a wheelchair changed my world overnight. I’ve been able to go on family outings, visit local parks and enjoy trips out to local shops. It means I can save my energy and pain levels from increasing through walking and use them on enjoying myself instead. I still sometimes feel awkward around family and people I haven’t seen in awhile – but if they can’t accept your need to get around without agonising pain – that’s their problem.
So if you’re sitting at home still trying to make that decision and thinking of the negatives – try to think of all the positive things you could do that you haven’t been able to do in some time if you’ve struggled with walking. A wheelchair could open more of the world to you.
My wheelchair – an Invacare TDX

by The Chronic Chronicles | Jan 22, 2014 | Benefits, Opinion
Yesterday I had an assessment by Social Services for Direct Payments. I’d been waiting about seven months for it after being assessed as ‘Urgent’. The Social Worker was fine – we talked through my condition, how it impacts me, the average day and what help I need.
What I did find interesting during the assessment is that after I was asked to give an overall idea of the help I’d ideally like – she then gave me a list of everything that my Disability Living Allowance was expected to cover, and so Social Services would not. From my list this included all cleaning, gardening, treatments not covered by the NHS, help with pets, and any activities even if they related to quality of life/better health and more.
As an aside, while I was aware of the cleaning issue, I am appalled that Social Services won’t help people with disabilities with cleaning at all. It’s not a cheap service to have, and I find it totally impossible to do such physical tasks as hovering, dusting, clothes washing, changing the bed sheets – and there’s people a lot worse than me out there. So they’ll pay to get you out of bed, and showered – then leave you in squalor to fend for yourselves?
But, back to my main point, I thought it was interesting how far she expected DLA to stretch. I currently use my DLA for an adapted car that has a hoist for my wheelchair. Without this, I couldn’t leave the house – as my wheelchair won’t go on buses, and wheelchair-adapted taxis are a rare sight to behold in my town (and usually double the price). Other people will often use this payment to hire a wheelchair from Mutability, or on taxis to get out and about.
Out of the rest of my DLA I and many others pay for things like extra heating, carers, mobility aids, therapeutic devices, special clothing/shoes, food that’s easier to cook (pre-prepared), the higher rents of accessible accommodation, medications, supplements, extra washing loads, specialist exercise programmes, special cushions, adapted items, insurance for wheelchair/scooter, petrol for additional car journeys (doctors/hospitals/travel to specialists often miles away, physiotherapists, other therapists, assessments as well as journeys most people would walk – but you have to drive instead) and so much more.
Of course people with disabilities are statistically more likely to be on a lower-income than the average person, even when able to work. So DLA may also help towards rent, bills and normal day-to-day living costs.
When I was trying to obtain an electric wheelchair through the NHS, as I am physically unable to manually propel – I explained I was using my Mobility Payments on a car that I needed to get to work. The assessors response was that I should be using it on a wheelchair. I pointed out that if I used it on a wheelchair and gave up my car, the wheelchair would have to live in the garden – and I would have to live on the sofa, as the car was vital in transporting the wheelchair, so what would be the point of that? She had no answer. It seemed it was their policy to be telling people to spend the DLA on wheelchairs too.
But it doesn’t cover a fraction of the extra costs I have for being disabled, and while I totally understand there isn’t a limitless supply of funds – it doesn’t help when agencies are putting more and more strain onto the benefit. Exactly how far do they expect DLA to go?
by The Chronic Chronicles | Jan 8, 2014 | Hospitals, Treatment
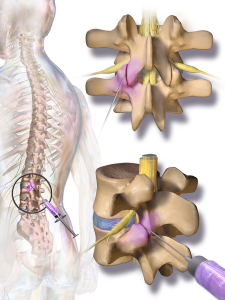
I have pain all over the place, but ranking at the top of the list is my lower back. I’d previously had facet joint injections in my neck and shoulders some years ago, but they didn’t help. However, it was before I’d had an MRI (as it took around 8 years of arguing to get one) and so the consultant was ‘guessing’ at what the issues were. Later on the MRI did clearly show an area in my lower back that had degenerative lumbar disease in the facet joints, arthritis, and others issues. It made a much better target for injections than anywhere else, so I thought it was worth a try.
It took another few years of me arguing for them (nothing ever just seems to just happen on the NHS!) After getting nowhere locally, my Ehlers-Danlos specialist at the Royal National Orthopaedic Hospital at Stanmore sent me to see her Pain Management college, who gave me the go-ahead for bilateral lumbar facet joints at L4/L5 and L5/S1 (so four in total).
A few days passed after being told I could have them and suddenly I thought – what the hell am I doing fighting to have needles put into my spine?! I was sedated during my previous injections, but I did have some memories of the procedure. I remember my consciousness kind of returning and thinking ‘please stop now.’ I was later told the sedation didn’t actually knock you out, but simply wiped your memory – and that you would be aware of what was happening as they did it. This memory built up in my mind until I was convinced I’d be strapped down with horrible painful injections into the middle of my spine, then I’d just forget afterwards so I didn’t realise how awful it would be. So I was about 500 times more nervous for these injections than previously.
The whole topic became a ‘do not discuss’ subject. As soon as I thought about it I went into a state of panic, so there was no research done as I normally would, and I didn’t even allow my mum (who accompanied me) to talk about our arrangements of getting there until the day before. I just wanted to block it totally from my mind.
We travelled to Stanmore the day before for two reasons. The first that I can’t make the journey there and back in one day, and the second was that my admission time was 7am. Ugh!
Although I wasn’t having general anaesthetic, I was told not eat after midnight, and no drinking after 6am. It was the latter I’d struggle with as I’m constantly thirsty.
I arrived at the hospital a couple of minutes before 7am and had a choice of parking for the first time ever! When we reached admissions there were a few people waiting outside, but when the queue got the doorway I realised the room was packed with both people queuing, and waiting in the chairs. It wasn’t the easiest getting my wheelchair in and out with no room for manoeuvring. There was only one member of staff dealing with everyone. The older lady in front of me didn’t speak any English, and was soon joined by an interpreter. The staff member made a phone call and I heard him say, “Are the wards still closed, there are a lot of patients here?” He then informed the interpreter they had a bit of a wait ahead. I was next, and was told the same thing.
I was a little cross, only because getting somewhere for 7am isn’t very easy for me and more importantly 7am = grumpiness! I did later found out the wards were opening for the first time after being closed for two weeks over Christmas – so I assume the delay isn’t normal.
I reached the ward and was met with a number of friendly nurses and health care assistants who welcomed me, and showed me my bed. The lady with the interpreter was in the bed opposite me. A nurse admitted me with a huge pile of paperwork, most of which seemed irrelevant in my case! I was asked a couple of times if I had any allergies. She then took swabs for MRSA and then took my blood pressure (which I hate, as it’s very painful. The muscles in my upper arm are very tight and particularly sensitive). I was told I was third in the queue – and the doctor would be seeing me beforehand.
A couple of other patients got in the bed and went to sleep, which seemed like a good idea – and would also make the time pass. However every time I was about to drift off I was woken by someone. The first to measure me for pressure stockings, then again to tell me I didn’t need them. Then a doctor who was working with my consultant arrived to explain the procedure. I was glad it was her and not my consultant as she was much warmer than my consultant is, which helped. She spent a lot of time explaining how much time they took to sterilise everything to reduce any chance of infection. I wanted to rudely interrupt and say that at that point, I didn’t care – I just wanted her to promise she’d knock me out! She then went through the possible risks – infection, numbness in the legs, pain flaring up afterwards and in a very tiny amount of cases nerve damage. She asked if I had any allergies.
Finally I could ask the one thing I wanted to know.
“You will be sedating me, right?”
“Did you ask for it before?”
“Yes,” I emphasised.
“Then we will.”
“Will I know what’s happening?”
“Well, some people do sleep.”
“Please make that happen with me. Please.”
Then the pharmacist came to take note of my list of medications, and asked whether I had any allergies, then a number of nurses came to tell me, “It won’t be much longer.” Then that they were on their way for me, only to still be there sometime later!
Eventually the porters did arrive and wheeled me into theatre. A nurse went through the final questions – checking I knew what procedure I was having, if I’d had any before, if I had any allergies and if it was definitely my signature on the consent form. The nice doctor then fitted the cannula into my hand, before I lay down front-first on the table. They put an oxygen mask on me, a clip onto my finger to measure oxygen (I’m sure that has a proper name) then to my annoyance – a blood pressure cuff which I was told would be taking my blood pressure every few minutes. It took it twice, before I told the nurse how painful it was. “No problem,” she told me cheerfully, and moved it onto my leg instead which was much better. She then began chatting to me about my hobbies and jewellery making, before my consultant began putting the sanitising fluids on my back. The nice doctor then began to input two injections of sedation into the cannula. I closed my eyes – trying to relax. She then asked if I could still hear her, and I said yes. She thought I’d gone to sleep, and I said I hadn’t felt any sedation yet. She said she’d keep going, and added two more tubes.
The next thing I remember is feeling a bit of pain in my back, and a nurse telling me it was all over. I definitely hadn’t been aware of it. I was taken into recovery for awhile, still very sleepy and groggy. A nurse chatted to me for awhile, and I remember telling her to say thank you to the nurses, as they’d calmed me down a lot beforehand. She promised she would. She then asked if I knew which ward I’d been in.
“It began with J…” I answered.
“Jackson Burrows is the only ward beginning with J.”
“No, it wasn’t that. Was it Diane something?”
“I guess now wasn’t the best time to test your memory?” she laughed. She then came back and said that unfortunately they’d moved me to Margaret Harte Ward. I began to worry if anyone had told my mum as I knew she was planning on getting a cup of tea while I was in the theatre (as she’d very kindly not eaten/drunk anything in front of me while I couldn’t).
As the porters wheeled me out of recovery, the nurse suddenly called for them to stop. She dug through a cupboard, and pulled out another blanket to put around me. “Sorry,” she said to the porters. “I just didn’t want her to get cold on the way back.”
When we got back to the ward I spotted my mum very quickly and realised it was the ward I’d been in all along! The nurse handed over to the ward nurse, and said that my blood pressure had risen quite a bit during the procedure, so they needed to keep an eye on it. Argh, more blood pressure checks!
I was left to sleep for a bit as I slowly came round. A nurse then came round to do the blood pressure test. I admit I groaned, and said the test was hurting quite a bit, then of course after gritting my teeth the machine malfunctioned. Just one more time, I was told. Luckily it was back to normal, and as she took the cuff off she realised lots of red marks had come up all the way round (which are still there today!). She gave me an apologetic pat. I asked if she could take my cannula out as it was pulling quite a bit. She took a look and said it was quite red, and that someone would do it before I left. (Well, one would hope so!)
I was told to stay until lunch time, and then I would be discharged. The nice nurse who admitted me then walked past and so I asked her about the cannula, and she said no problem and took it out. She also checked my ‘wounds’ (just slightly larger than needle marks) and said she was happy with how they looked.
Still waiting opposite me was the older lady with the interpreter. I heard a nurse say to her that her operation wasn’t going to be until mid-afternoon – yet she’d been admitted at 7am! It seemed mean to make her wait so long, and I assume the NHS had paid extra for the interpreter when they could had admitted her at the 11am or 2pm admission times. I noticed the little old lady chatted non-stop to her interpreter, which made me smile as I could just imagine in the 7+ hours the interpreter sat with her she got to hear her entire life story.
I left at 1:40pm, slept all the way home, slept all afternoon and very unusually for me – all night!
So all in all – it wasn’t nearly as bad as I dreaded. The staff – particularly the nurses, were lovely. There were lots of touches of kindness, like the nurse in the theatre distracting me from my nerves, the recovery nurse chatting to me as I came round and making sure I was warm, and the staff back on the ward who took care of me and offered me toast and regular drinks when I came round. They all made it a much easier experience. Also – the NHS really, really want to know if you have any allergies.
I’m in a lot of pain now which feels different to my usual pain. I was warned I may flare up, particularly where the needle touches the bone – so I’ve no idea if it worked yet. I think I need to wait for all of that to calm down over the next couple of days before I can tell if it helped.
An image of a facet joint injection

by The Chronic Chronicles | May 23, 2012 | Coping Methods, Vents
If you ask a doctor how to care for a chronic condition, or read their guidelines, or even go in hospital for a month on an intensive-pain management course (just to be specific) the themes running through them all, their little buzzword, is self-care.
I was reading the papers that have been created in the wake of the imminent closure of the PCTs by the doctors commissioning consortia whose priorities for the future are self-care, with aims to give patients the confidence to manage their conditions themselves.
To be fair, this may help with some conditions where perhaps a specific therapy or medication keeps symptoms at bay, but it gets a little more complicated when it comes to complex conditions where pain and fatigue are two pervading symptoms, amongst many others, because there is no single treatment. There isn’t even ten treatments they can say hand on heart would help everyone with chronic pain.
To be frank, it infuriates me to hear phrases such as ‘take control of your own treatment’ or ‘You have the power in your hands’ etc, etc, blah, blah, blah.
What they don’t tell you is that you have to. Self-care, that is. Because it will make up 99.9% of your overall treatment plan. Oh, it may be occasionally the NHS will think of something – physiotherapy injections, uhh… more physiotherapy, that is if you kick up enough fuss. Otherwise, it’s DIY all the way.
At the age of 15 I visited a Rheumatologist. He said I’d ‘grow out of it’. In the following years I was sent a couple of times for Physiotherapy, but it didn’t make the slightest bit of difference. The NHS then gave up, and in desperation I saw chiropractors, osteopaths, acupuncturists and electro-acupuncturists. I tried the many sheets of exercises and stretches, swimming and pilates and a GP referral to the gym (that I paid for) which put me in bed for two weeks. I then started the ‘alternative’ stuff like the Alexander Technique to improve posture, the Bowen Technique which seemed weird and pointless. I saw Kinesiologists and had relaxation sessions. The only tiny bit of relief came from the many thousands of massage treatments I once again paid for.
I’ve researched madly, kept up to date with papers on pain, studies on medication, and constantly visit the doctor with a new research paper in hand.
I even diagnosed myself – after years of consultants shrugging their shoulders at me, I kept searching and searching until I finally realised what was wrong with me, and then fought to see consultants in London who finally knew what they were talking about.
I now can only exist and function from a mixture of massage and adjustments, which takes the edge off – maybe 5-10% at best. But it’s an important percentage.
In the ten years I’ve been madly trying anything and everything, the NHS gave me one set of facet joint injections in 2008. Some muscle injections in 2011. And six sessions of Hydrotherapy – but I had to fight for them all.
The thing I find infuriating is that no one tells you exactly what IS available. I had severe back problems for ten years before someone said to me there was a spine clinic in my town for people with long-term back issues. Do you really have to hit the ten year mark before they go crap, that is long term for a twenty-four year old?
When you get a diagnosis no one gives you a handbook and says here is what the Pain Clinic offer (if they deem you lucky enough to offer you anything at all) or let you know you can see Osteopaths and Chiropractors on the NHS. Or any other of the treatments they may have available. You have to wait until you stumble upon it yourself.
All they do is hand out painkillers (again, if you are lucky) and tell you self-care is the way it should be.
Sometimes I want to say you know what? I’ve self-cared. NHS – it’s your goddamn turn. I’m just too tired.

by The Chronic Chronicles | Nov 8, 2011 | Opinion
The NHS is currently under threat from something called the ‘Health and Social Care Bill 2011’.
The bill will make many changes, including abolishing Primary Care Trusts (PCTs) and grouping together GP groups to run their area. While we hope GPs are making decisions based on the patient, they are much more likely to be influenced by finances under the changes. I also hope my GP is spending her time reading the latest research, keeping up to date with training and new medications, not budgeting for the local area. It will allow private companies to take over NHS hospitals, or the services that appeal to them and will stop the NHS being the comprehensive service it should be.
20% of the NHS budget will be spent on things like dealing with the contracts with private companies, advertising, the legal bits that go along with contracts, and a lot of other stuff that isn’t providing quality healthcare or trained staff. Many people will be made redundant – with payments having to be made, and those running the PCTs are likely to then be employed to be consultants to the GP groups.
The postcode lottery that already exists will become even more pronounced, with standards and range of care dependant on where you live. Hospitals will be able to treat more private patients, which seems okay in principle into you need the bed someone who can afford to pay for one is in.
It is one thing if you have an injury and go to A&E to be fixed, or you need a single operation like a knee replacement. The difficulty comes when people are chronically ill, such as myself. With these conditions come all sorts of problems, in different parts of the body, and there is no one specialist that can help me. At the moment my GP can refer me to a variety on consultants, and I currently see six consultants on a regular basis, in different parts of the country.
Under the new plans – the person I want to see may now be available only if I can afford to pay for it, which goes against the very philosophy of the NHS – free care, from cradle to grave.
Debates will be happening soon on Clause 4 of the NHS Bill, also known as the “hands-off clause.” It will completely change the way the minister’s duties towards the NHS, and mean they will only be able to stop something happening, or bring a change in, if they can demonstrate there was no other course of action. This isn’t very easy to do. The NHS is one of the most important issues for voters, and they are expecting ministers to try and take care of it – not sign a bill waiving away their responsibility. More information on this clause can be found here.
The government did not state in their manifesto they would be making these changes, and public support is largely against it, yet they seem to be pressing forward with them.
I’ve been trying to follow the 38 Degrees campaign, who have taken petitions to hundreds of MPs, including Nick Clegg, send thousands of emails, and are now asking people to ‘email a Baroness Lord’ at random to ask them to attend the debates. My pick is Baroness O’Neill, so I will be emailing her to tell her why I don’t support the bill.
You can do the same here.
Credit to Grafixar