by The Chronic Chronicles | Jan 9, 2015 | Doctors
Credit to Kurhan
Yesterday I went to London to see Dr Hakim, one of the top specialists in Britain for Ehlers-Danlos Syndrome.
I was nervous when I got there – I always am before I see a consultant, due to many, many bad experiences. However he immediately put me at ease, and was a nice, approachable person.
I’d made a list of problems I wanted to talk about, and he made a note of them and went through each in turn giving me ideas and suggestions of particular treatments or medications I could try.
He said in terms of exercise I was doing everything right, and everything I could. This meant a lot, as I’ve had medical professionals be so judgmental with no understanding of how hard it is to do the ‘little’ I do without putting myself in bed for weeks. I told him what one Pain Consultant had said – that I should be exercising six times a day. He said it was such an easy thing to say, and proved how little he knows.
We spoke about my Physiotherapist Leon Stephens at Sudbury Physiotherapy Centre who specialises in Hypermobility, and has been great, and Dr Hakim knew of him, which was good.
At some point this year I need to renew my Employment and Support Allowance, and in the next couple of years my indefinite Disability Living Allowance award will be changed over to the replacement – Personal Independence Payment (PIP). I’m terrified about both of these, as are most disabled people in the country who currently rely on them – or may need them in the future – to survive. I never know how people may react to something like that, due all the ‘scroungers’ rhetoric in the media, that has been picked up by so many.
Since I received my diagnosis letter in 2011 – I haven’t had a decent letter from a consultant that I could use as medical evidence. I’ve seen lots of consultants, but letters are generally of the “Treatment x didn’t work, been discharged” variety which won’t help much in terms of summarising where I’m currently at on the whole. I feared the lack of letters may go against me, as the Department of Work and Pensions will argue I can’t be that bad if I don’t see a consultant regularly.
Dr Hakim was very understanding of this, and we spoke at length about the PIP changeover, and he knew how hard it was on his patients. He said it’s obvious the reason I don’t have new evidence is because I’m doing the best I can at home to manage, but he would write an updated version for me to keep on file for when I need this.
This will take a huge worry away from me, so I’m thrilled.
He recommended that I take a multivitamin daily – he mentioned the Well Woman one, to make sure I’m topping up on anything that could be contributing to my levels of fatigue. He’s also going to ask my GP to check every blood test has been done, including the T3 Thyroid test that the NHS often miss out. He also suggested getting some Melatonin from the US, as well as suggesting some other sleep and pain medications I have yet to try that he’s going to suggest to my GP to look into (I can’t remember the name of them currently!) He also recommended some consultations in other fields that I could see if I continue to get nowhere locally.
He also suggested that anyone with POTs or autonomic dysfunction (including sleep problems) to drink an Isotonic drink called Nuun. He explained that they tell people like us to keep hydrated, so we drink water – but it actually make things worse as it dilutes the salt in our blood, so our kidneys then filter it and we pass it out with urine leaving things actually worse. (Or something like that!)
So he suggested drinking a salt isotonic drink which means that we are really hydrated, as drinking liquid with a similar salt content as our blood means it will do its job, rather than being filtered and disposed of straight away. Most of the similar products on the market i.e. sports drinks, Lucozade, etc are full of crap and sugar, so he suggests Nuun as it doesn’t add much else, just some flavouring. He suggested at a minimum to drink one before bed, and one as soon as you wake up, and this should stabilise some of those issues.
They are pretty expensive, but we only need half a tablet at a time, as the whole tablets are designed for athletes.
We also spoke about Prolotherapy, which is a new therapy I’m hearing a lot about recently, mostly from Americans, and I was interested in his thoughts. He said there was no evidence for it, and some of his patients had been made worse by it.
I found Dr Hakim very understanding, kind and obviously knowledgeable. All in all it was a great appointment – and when his letter arrives I will add anything helpful I’ve forgotten!
Professor Grahame retired from NHS patients some time ago, and is no longer taking on new private patients. I believe he may still have a private clinic for under 16s, but Dr Hakim is a perfect alternative.
by The Chronic Chronicles | Feb 28, 2014 | Awareness, Education
There are lots of these special ‘days’ – Talk Like a Pirate Day (19th Sept), Hairstyle Appreciation Day (30th April) and National Sandwich Day (3rd Nov) but a really important day for me is Rare Disease Day, which is today.
A disease is defined as a condition that’s abnormal, and affects the body of a living being.
Here are some facts about rare diseases:
- There are over 6000 rare diseases
- A disease is classed as rare if it impacts fewer than 1 in 2000 people
- 30 million people live with a rare disease in Europe
- 80% of rare conditions have a genetic origin
I have Ehlers-Danlos Syndrome, a genetic connective tissue disorder.
There are various types of the condition and the most common type is estimated to impact anywhere from 1 in 5000 to 1 in 10,000 and the least common types have only been diagnosed with a small handful of people.
Rare diseases are neglected – in research, care, NHS services and provision of medical expertise. There is a lack of understanding and awareness in every part of the medical community. But rare doesn’t mean we don’t matter.
While I had mild symptoms from birth, the real trouble started when I was 15 – and it took me another eight and a half years to be able to put a name to my pain, fatigue and countless other symptoms. I’m lucky – many others don’t get diagnosed at all. That’s why recognition is vitally important.
Many seeking answers are instead labelled incorrectly. The word hypochondriac sneaks into their medical notes. They’re told their attitude is too negative, or point-blank informed it’s all in their heads. People with the condition usually look perfectly healthy, which makes it even easier to get dismissed.
Some people don’t live long enough to have the reassurance of knowing they were completely right, and there was a reason they felt the way they do like in this awful story.
Once I knew what was wrong with me, it changed everything. I was able to look for the national charities, find other sufferers and do copious amounts of research. Everyone should be able to do that – and from as near to birth as possible. Simple changes like strengthening your muscles before they become locked in a cycle of spasms, wearing orthotics to protect flat feet and looking out for the myriad of complications that can arise from the condition can make a big difference.
Awareness for rare conditions isn’t the same as for many other conditions. To me it can be summed up in the conversation that usually goes,
“So what’s wrong with you?”
“Ehlers-Danlos Syndrome.”
And the response is a blank face.
I don’t expect people to know specifics – but if you said to someone you had MS, they’d probably at least gather it’s quite debilitating without having to try to explain further.
While that may not feel so bad – imagine that lack of recognition continues with your GP, your rheumatologist, physiotherapist – the people meant to be supporting your care, as well as everyone else. You have to spell the words out to them carefully, and they promise they’ll look it up – but yet the next time you see them they’re none the wiser, and you know they forgot to pop it into google. We deserve better, and it makes you feel very alone.
When I was diagnosed I spent an hour with the specialist consultant. He was the first person who nodded when I mentioned symptoms, and pointed out a lot I hadn’t even realised were significant. He literally started from when I was born onwards, and put together a pattern that led to my diagnosis.
However, an hour isn’t enough -not when you’ve just been diagnosed with a condition that impacts 95% of your entire body. Every organ, every joint. No one talked me through the heart issues, the gastrointestinal problems, bladder, muscle tone, nervous system, eye sight, breathing issues , and the terrible sleeping problems. No one told me that while you’re given a ‘type’ within the condition – there’s lots of overlap, and it’s mostly just guess work.
To this day I’m still finding new information, and putting facts together – and I usually find that out from other people with the condition, not a medical professional.
So this is what I want from Rare Disease Day…
I want every medical professional to have a brief understanding of the condition, and realise it’s only rare because they aren’t spotting all the undiagnosed people with it. Professor Grahame, a Ehlers-Danlos Syndrome specialist consultant carried out research that suggested “for every one person in England who is diagnosed by a rheumatologist as having hypermobility syndrome, there are probably 19 that aren’t yet diagnosed.” That’s around 85% of cases that are going untreated, being told it’s in their head, or being misdiagnosed. This has to change.
The most common sign of Ehlers-Danlos Syndrome is hypermobile joints – something that should be second nature for GPs/physiotherapists to have a quick look for if someone is presenting with wide-spread pain. I first heard the word hypermobilty from a physiotherapist I was lucky enough to come across. She asked me if I knew I was hypermobile, and I said I didn’t know what she meant. She explained it was also known as being double-jointed, but the only time I’d ever seen people mention that was when people did funny tricks with their hands. My hands looked normal. “Of course you’re hypermobile,” the physiotherapist said to me. “Just look at you, look at your toes, you just are!”
That’s all it takes. One person to have the knowledge. To be able to spot hypermobile joints, to notice the person with pain in every joint that is getting negative results to every test, to the person gesticulating with their hands as they speak, with bruises or injuries they don’t remember getting, that might be a bit clumsy. If you spot just one of those things, just have a think about mentioning Ehlers-Danlos Syndrome and you might change someone’s life.
by The Chronic Chronicles | Jan 8, 2014 | Hospitals, Treatment
I have pain all over the place, but ranking at the top of the list is my lower back. I’d previously had facet joint injections in my neck and shoulders some years ago, but they didn’t help. However, it was before I’d had an MRI (as it took around 8 years of arguing to get one) and so the consultant was ‘guessing’ at what the issues were. Later on the MRI did clearly show an area in my lower back that had degenerative lumbar disease in the facet joints, arthritis, and others issues. It made a much better target for injections than anywhere else, so I thought it was worth a try.
It took another few years of me arguing for them (nothing ever just seems to just happen on the NHS!) After getting nowhere locally, my Ehlers-Danlos specialist at the Royal National Orthopaedic Hospital at Stanmore sent me to see her Pain Management college, who gave me the go-ahead for bilateral lumbar facet joints at L4/L5 and L5/S1 (so four in total).
A few days passed after being told I could have them and suddenly I thought – what the hell am I doing fighting to have needles put into my spine?! I was sedated during my previous injections, but I did have some memories of the procedure. I remember my consciousness kind of returning and thinking ‘please stop now.’ I was later told the sedation didn’t actually knock you out, but simply wiped your memory – and that you would be aware of what was happening as they did it. This memory built up in my mind until I was convinced I’d be strapped down with horrible painful injections into the middle of my spine, then I’d just forget afterwards so I didn’t realise how awful it would be. So I was about 500 times more nervous for these injections than previously.
The whole topic became a ‘do not discuss’ subject. As soon as I thought about it I went into a state of panic, so there was no research done as I normally would, and I didn’t even allow my mum (who accompanied me) to talk about our arrangements of getting there until the day before. I just wanted to block it totally from my mind.
We travelled to Stanmore the day before for two reasons. The first that I can’t make the journey there and back in one day, and the second was that my admission time was 7am. Ugh!
Although I wasn’t having general anaesthetic, I was told not eat after midnight, and no drinking after 6am. It was the latter I’d struggle with as I’m constantly thirsty.
I arrived at the hospital a couple of minutes before 7am and had a choice of parking for the first time ever! When we reached admissions there were a few people waiting outside, but when the queue got the doorway I realised the room was packed with both people queuing, and waiting in the chairs. It wasn’t the easiest getting my wheelchair in and out with no room for manoeuvring. There was only one member of staff dealing with everyone. The older lady in front of me didn’t speak any English, and was soon joined by an interpreter. The staff member made a phone call and I heard him say, “Are the wards still closed, there are a lot of patients here?” He then informed the interpreter they had a bit of a wait ahead. I was next, and was told the same thing.
I was a little cross, only because getting somewhere for 7am isn’t very easy for me and more importantly 7am = grumpiness! I did later found out the wards were opening for the first time after being closed for two weeks over Christmas – so I assume the delay isn’t normal.
I reached the ward and was met with a number of friendly nurses and health care assistants who welcomed me, and showed me my bed. The lady with the interpreter was in the bed opposite me. A nurse admitted me with a huge pile of paperwork, most of which seemed irrelevant in my case! I was asked a couple of times if I had any allergies. She then took swabs for MRSA and then took my blood pressure (which I hate, as it’s very painful. The muscles in my upper arm are very tight and particularly sensitive). I was told I was third in the queue – and the doctor would be seeing me beforehand.
A couple of other patients got in the bed and went to sleep, which seemed like a good idea – and would also make the time pass. However every time I was about to drift off I was woken by someone. The first to measure me for pressure stockings, then again to tell me I didn’t need them. Then a doctor who was working with my consultant arrived to explain the procedure. I was glad it was her and not my consultant as she was much warmer than my consultant is, which helped. She spent a lot of time explaining how much time they took to sterilise everything to reduce any chance of infection. I wanted to rudely interrupt and say that at that point, I didn’t care – I just wanted her to promise she’d knock me out! She then went through the possible risks – infection, numbness in the legs, pain flaring up afterwards and in a very tiny amount of cases nerve damage. She asked if I had any allergies.
Finally I could ask the one thing I wanted to know.
“You will be sedating me, right?”
“Did you ask for it before?”
“Yes,” I emphasised.
“Then we will.”
“Will I know what’s happening?”
“Well, some people do sleep.”
“Please make that happen with me. Please.”
Then the pharmacist came to take note of my list of medications, and asked whether I had any allergies, then a number of nurses came to tell me, “It won’t be much longer.” Then that they were on their way for me, only to still be there sometime later!
Eventually the porters did arrive and wheeled me into theatre. A nurse went through the final questions – checking I knew what procedure I was having, if I’d had any before, if I had any allergies and if it was definitely my signature on the consent form. The nice doctor then fitted the cannula into my hand, before I lay down front-first on the table. They put an oxygen mask on me, a clip onto my finger to measure oxygen (I’m sure that has a proper name) then to my annoyance – a blood pressure cuff which I was told would be taking my blood pressure every few minutes. It took it twice, before I told the nurse how painful it was. “No problem,” she told me cheerfully, and moved it onto my leg instead which was much better. She then began chatting to me about my hobbies and jewellery making, before my consultant began putting the sanitising fluids on my back. The nice doctor then began to input two injections of sedation into the cannula. I closed my eyes – trying to relax. She then asked if I could still hear her, and I said yes. She thought I’d gone to sleep, and I said I hadn’t felt any sedation yet. She said she’d keep going, and added two more tubes.
The next thing I remember is feeling a bit of pain in my back, and a nurse telling me it was all over. I definitely hadn’t been aware of it. I was taken into recovery for awhile, still very sleepy and groggy. A nurse chatted to me for awhile, and I remember telling her to say thank you to the nurses, as they’d calmed me down a lot beforehand. She promised she would. She then asked if I knew which ward I’d been in.
“It began with J…” I answered.
“Jackson Burrows is the only ward beginning with J.”
“No, it wasn’t that. Was it Diane something?”
“I guess now wasn’t the best time to test your memory?” she laughed. She then came back and said that unfortunately they’d moved me to Margaret Harte Ward. I began to worry if anyone had told my mum as I knew she was planning on getting a cup of tea while I was in the theatre (as she’d very kindly not eaten/drunk anything in front of me while I couldn’t).
As the porters wheeled me out of recovery, the nurse suddenly called for them to stop. She dug through a cupboard, and pulled out another blanket to put around me. “Sorry,” she said to the porters. “I just didn’t want her to get cold on the way back.”
When we got back to the ward I spotted my mum very quickly and realised it was the ward I’d been in all along! The nurse handed over to the ward nurse, and said that my blood pressure had risen quite a bit during the procedure, so they needed to keep an eye on it. Argh, more blood pressure checks!
I was left to sleep for a bit as I slowly came round. A nurse then came round to do the blood pressure test. I admit I groaned, and said the test was hurting quite a bit, then of course after gritting my teeth the machine malfunctioned. Just one more time, I was told. Luckily it was back to normal, and as she took the cuff off she realised lots of red marks had come up all the way round (which are still there today!). She gave me an apologetic pat. I asked if she could take my cannula out as it was pulling quite a bit. She took a look and said it was quite red, and that someone would do it before I left. (Well, one would hope so!)
I was told to stay until lunch time, and then I would be discharged. The nice nurse who admitted me then walked past and so I asked her about the cannula, and she said no problem and took it out. She also checked my ‘wounds’ (just slightly larger than needle marks) and said she was happy with how they looked.
Still waiting opposite me was the older lady with the interpreter. I heard a nurse say to her that her operation wasn’t going to be until mid-afternoon – yet she’d been admitted at 7am! It seemed mean to make her wait so long, and I assume the NHS had paid extra for the interpreter when they could had admitted her at the 11am or 2pm admission times. I noticed the little old lady chatted non-stop to her interpreter, which made me smile as I could just imagine in the 7+ hours the interpreter sat with her she got to hear her entire life story.
I left at 1:40pm, slept all the way home, slept all afternoon and very unusually for me – all night!
So all in all – it wasn’t nearly as bad as I dreaded. The staff – particularly the nurses, were lovely. There were lots of touches of kindness, like the nurse in the theatre distracting me from my nerves, the recovery nurse chatting to me as I came round and making sure I was warm, and the staff back on the ward who took care of me and offered me toast and regular drinks when I came round. They all made it a much easier experience. Also – the NHS really, really want to know if you have any allergies.
I’m in a lot of pain now which feels different to my usual pain. I was warned I may flare up, particularly where the needle touches the bone – so I’ve no idea if it worked yet. I think I need to wait for all of that to calm down over the next couple of days before I can tell if it helped.
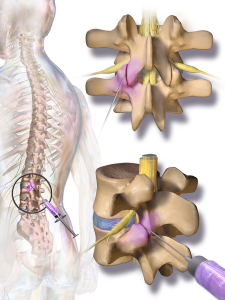
An image of a facet joint injection

by The Chronic Chronicles | Dec 23, 2013 | Hospitals
I stumbled across the treatment of ‘infusions’ sometime ago, and then kept seeing them being mentioned. I began to try to find out more about them, but information was limited.
I was aware it usually consisted of either Ketamine or Lidocaine being given by an IV, and for some it works really well for pain relief. For others it seems to do nothing at all.
Eventually a friend kindly offered to search the academic databases he had access to and sent me all the research he could find. They were generally all positive.
‘Intravenous Lidocaine: An Outdated or Underutilized Treatment for Pain?’ by Gary McCleane stated, “The drug is administered over a relatively short period of time and yet the potential relief lasts significantly beyond both the period of administration and the plasma half-life of this local anesthetic.” He goes on to state that, “an infusion over a few hours can produce relief that extends to weeks and even months. Consequently, side effects, if any are apparent, are short lived and last for a much shorter time than the pain relief.”
McCleane explained that for many patients undertaking this treatment it becomes their only form of pain-relief, and they’re able to stop all other medications for pain. A trial of 82 patients found that 82% had a very good pain reduction after their infusion. In a second study on people with Fibromyalgia it was found that 40% of patients had between 13-18 weeks of relief.
A second study called ‘Efficacy and adverse effects of intravenous lignocaine therapy in fibromyalgia syndrome’ concluded that the therapy “appears to be both safe and of benefit in improving pain and quality of life for patients with fibromyalgia.”
The one downside is that there wasn’t much research on the therapy, and when a study had taken place they had very small sample sizes. There are also side effects such as hypotension, tachycardia, infections and other such fun times.
I began by asking my GP about them, but she’d never heard of them. I asked at the various London hospitals I’m under, but was told they didn’t do them. I came across a number of people with Ehlers-Danlos Syndrome who’d had them, but it was never at a hospital near to me.
I then visited a pain clinic in another town but they too stated they didn’t do them, and if they did they wouldn’t do it for Ehlers-Danlos Syndrome as there weren’t enough of us with it. (Red flag to a bull!)
I then changed GPs, and she too hadn’t heard of them – but a few weeks later I got a phone call from her. She explained she’d just had a patient in to see her who’d just had infusions at the hospital in my own town! She told me to come and see her, and she’d get me referred.
I saw a consultant at the pain clinic last week and she agreed I could have one infusion. I’m not sure why just one, but still it’s good news!
I’m also due to have facet joint injections in January, so there are two treatments coming up that allow me to have some hope.
An IV
Credit to: andyk

by The Chronic Chronicles | Oct 16, 2013 | Doctors
By 2010 I’d seen a string of consultants over the years, but none had been able to tell me what was wrong. They’d all been appointments of around 15 minutes, a quick look at my spinal movement, a couple of questions , a shrug of their shoulders and a dismissal. I left each appointment feeling lost and disappointed.
A physiotherapist then mentioned I was very hypermobile, which then put me on a path of research into what that meant, the implications and I then came across the condition Ehlers-Danlos Syndrome which seemed to fit all my symptoms. I also found that one of the top specialists in the condition, Professor Rodney Grahame, was based at the University College Hospital London.
I then had quite a fight to get the referral, having to go through the PCT and Rheumatology department at my local hospital – but finally I was informed they were willing to refer me for a second opinion and I had the funding for it.
It took about six months until I saw Professor Grahame, in January 2011. I knew he was different when he began to put together a detailed overview from my birth to the current day. I was with him for over an hour – and he was very thorough and polite. He explained what was wrong with me, and some of the things I could try – including referrals to other specialists. I felt listened to, respected and finally had the answers I had been seeking for so long. He also followed my appointment up with a very detailed report that helped me secure further support from other sources.
I saw him again eighteen months later for a follow-up, where again he was very helpful, and enabled me to have further testing within weeks, that I’d been asking for locally for the past two years.
Sadly, Professor Grahame retired this year and it’s a massive setback for the Ehlers-Danlos Syndrome sufferers in the UK. There is a shocking lack of specialists and clinics in the UK – and Professor Grahame has been unfailing in his research and support. He changed the lives of so many families by finally being able to give answers to people sometimes after decades of uncertainty. He brought a particular kindness and expertise that many others lack.
He will be sorely missed at the UCHL, but I hope he enjoys his retirement!